 VISIT STATE HEALTH COMPARE
VISIT STATE HEALTH COMPARE
Blog & News





NHIS: Uninsurance Rates Held Mostly Steady in First Half of 2017 but Increased among Key Subgroup
February 22, 2018:Recent Gallup polls have shown adult (18+) uninsurance rates increasing in 2017, leading many to wonder whether federal survey data would show a similar jump in uninsurance. However, new coverage estimates from the National Health Interview Survey (NHIS) indicate that uninsurance rates for nonelderly adults (18 to 64) held steady in the first half of 2017.
| Why the Differing Stories about Uninsurance? | |
|---|---|
|
The Gallup poll measuring uninsurance and the National Health Interview Survey employ different methods, instruments, and definitions in generating their respective estimates. As a result, their findings are not directly comparable. |
According to the new numbers, 12.5% of nonelderly adults nationwide were uninsured during the first half of 2017, which is statistically unchanged from 12.4% during the first half of 2016.
This stability in NHIS estimates of uninsurance from 2016 to 2017 mirrors the stability seen from 2015 to 2016, which was preceded by historic declines from 2013 to 2014 and from 2014 to 2015.
The new NHIS estimates also show that uninsurance rates were mostly stable across age, race/ethnicity, and income groups when comparing the first half of 2016 to the first half of 2017. There was, however, an exception to this stability: Among nonelderly adults (18 to 64) with incomes between 250% and 400% of the federal poverty level (FPL), the uninsurance rate increased significantly from 10.2% to 12.2%. This is an important subgroup from a policy perspective, because people in this income range are among the population (100% to 400% FPL) for whom the ACA's individual market provisions specifically aim to expand coverage. During the 2017 open enrollment period, individuals between 250% and 400% FPL made up nearly 20% of consumers enrolling in marketplace plans on HealthCare.gov.
| Uninsurance: Disparities among Subgroups in 2017 | |
|---|---|
|
Disparities in uninsurance levels continued to be seen among certain subpopulations in the first half of 2017:
|
Increased Enrollment in High-Deductible Health Plans
When comparing data from the first half of 2016 with the first half of 2017, some shifts in public and private coverage emerge.
The percentage of nonelderly Americans enrolled in high-deductible health plans (HDHPs) was one of the few broad points of change in the NHIS estimates, increasing significantly between the first half of 2016 and the first half of 2017, from 38.8% to 42.9% (4.1pp). This increase was even more pronounced among individuals with employer-sponsored insurance, among whom the percentage enrolled in HDHPs jumped from 38.7% in the first half of 2016 to 43.5% in the first half of 2017 (4.8pp).
Private and Public Coverage Rates Changed in Some Cases
| More about Those High-Deductible Health Plans... | |
|---|---|
|
The trend of increasing enrollment in HDHP plans through an employer echoes the findings from SHADAC’s recent in-depth analysis of employer-sponsored insurance coverage from 2015 to 2016. Learn more. |
- Private coverage rates increased significantly from 21.6% to 25.8% for nonelderly adults (18 to 64) below the federal poverty level and from 16.1% to 19.4% for all nonelderly individuals (0 to 64) below the poverty level.
- Private coverage rates decreased significantly from 82.7% to 80.3% among children (0 to 17) with incomes at or above 200% of the poverty level and from 84.4% to 83.2% among all nonelderly individuals (0 to 64) with incomes at or above 200% of poverty.
- Public coverage for children at or above 200% of the poverty level increased significantly from 15.1% to 17.3%.
Uninsurance Gap between Medicaid Expansion States and Non-Expansion States Persists
At 8.8%, uninsurance in the first half of 2017 continued to be significantly lower among nonelderly adults (ages 18-64) in states that expanded Medicaid than in states that did not expand Medicaid, where the uninsurance rate for this group was 19.0%.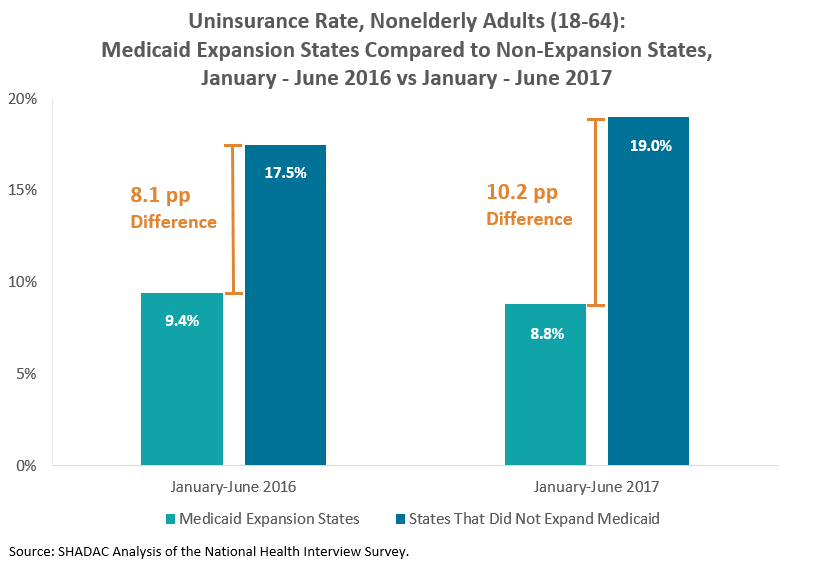
The gap between uninsurance levels in expansion and non-expansion states for the first half of 2017 was wider than the gap seen in the first half of 2016 (see figure above), as was the case when comparing the first quarters of 2017 and 2016. We will continue to track the size of this gap as additional NHIS data are released.
A Note about the Numbers
The above estimates provide a point-in-time measure of uninsurance, indicating the percent of persons without coverage at the time of the interview. First half of the year refers to January through June.
For more information about the early 2017 NHIS health insurance coverage estimates, read the NCHS brief. Estimates for the first half of 2016 are available here.
Citation
Zammitti, E.P., Cohen, R.A., & Martinez, M.E. November 16, 2017. “Health Insurance Coverage: Early Release of Estimates from the National Health Interview Survey, January-June 2017.” National Center for Health Statistics: National Health Interview Survey Early Release Program. Available at https://www.cdc.gov/nchs/data/nhis/earlyrelease/insur201711.pdf
Blog & News
How Do State Policy Decisions Impact Out-of-Pocket Spending & Health Insurance Coverage? SHARE Panel at APPAM
October 30, 2017:![]() Findings from three SHARE-funded analyses will be the focus of a panel session at the 2017 APPAM Fall Research Conference in Chicago.
Findings from three SHARE-funded analyses will be the focus of a panel session at the 2017 APPAM Fall Research Conference in Chicago.
The panel, "How Do State Policy Decisions Impact Out-of-Pocket Spending & Health Insurance Coverage? Evidence from Federal Survey Data," will feature the following presentations:
- The Impact of Medicaid Expansion on Employer Provision of Health Insurance
Anne Royalty, Indiana University - Medicaid vs. Marketplace Coverage for Near-Poor Adults: Impact on Out-of-Pocket Spending Burdens
Fred Blavin, Urban Institute - Do Minimum Wage Changes Affect Employer-Sponsored Insurance Coverage in the Post-ACA Era?
Michael Dworsky, RAND Corporation
All three papers on the panel use federal survey data to consider the impacts of state policy choices on health insurance coverage and/or spending. The first paper uses data from the Medical Expenditure Panel – Insurance Component (MEPS-IC) to investigate how employer insurance offers, workers’ eligibility, and out-of-pocket premiums are changing as a result of state Medicaid expansion decisions. The second paper uses data from the Current Population Survey (CPS) to examine the comparative out-of-pocket spending burdens for adults with incomes between 100 and 138% of the federal poverty level (FPL) in states that have chosen to expand Medicaid—where this group faces little to no cost-sharing in most cases—and in states that have chosen not to expand Medicaid, where this group may face out-of-pocket premiums and cost-sharing for coverage purchased through the marketplace. Finally, the third analysis uses CPS data to examine the impact of recent state minimum wage increases on enrollment in employer-sponsored insurance (ESI) coverage and considers whether the impact of the minimum wage changes varied between Medicaid expansion states and non-expansion states.
SHADAC Director Lynn Blewett will moderate the panel session, and SHADAC Investigator Kathleen Call will act as the panel discussant.
This panel will take place on Saturday, November 4th, 3:30-5:00 p.m., in the Hyatt Regency Chicago Toronto Room.
Publication
Comparing Federal Government Surveys That Count the Uninsured: 2017
This brief provides an annual update to comparisons of uninsurance estimates from four federal surveys1:
- The American Community Survey (ACS)
- The Current Population Survey (CPS)
- The Medical Expenditure Panel Survey - Household Component (MEPS-HC)
- The National Health Interview Survey (NHIS)
In this brief, we present current and historical national estimates of uininsurance along with the most recent avaialble state-level estimates from these surveys. We also discuss the main reasons for variation in the estimates across the different surveys.
1Another federal survey that provides estimates of the uninsured is the Behavioral Risk Factor Surveillance System (BRFSS), which provides uninsurance estimates for the adult population 18 years and over nationally and among states. Details about the BRFSS are included in Appendix A of the brief, and estimates from the BRFSS are provided in Appendix B.
Blog & News
Now Available: 2016 State & County Uninsured Tables, with Comparison Year 2015
September 18, 2017:
SHADAC has produced tables of state and county uninsurance estimates for 2016 and comparison year 2015. These estimates come from the 2016 American Community Survey (ACS) via the U.S. Census Bureau's American FactFinder (AFF) tool and were released on September 14, 2017.
SHADAC's tables provide uninsured rates by characteristics (e.g., age, race/ethnicity, and poverty level) for both 2016 and comparison year 2015 for each state (and the district of Columbia and Puerto Rico) and for all counties within each state that have a population greater than 65,000. The tables are available via clickable map here.
Additional Tables: Private, Public, & Uninsured Change from 2015 to 2016
SHADAC has created the following 50-state comparison tables (with maps) in addition to the state and county uninsured tables:
- Private Coverage Rates by State, Change from 2015 to 2016, for All People
- Public Coverage Rates by State, Change from 2015 to 2016, for All People
- Uninsurance Rates by State, Change from 2015 to 2016, for All People
Publication
2016 ACS Tables: State & County Uninsured Rates, with Comparison Year 2015
The map on this page links to tables containing state and county uninsurance estimates for 2016. These estimates come from the 2016 American Community Survey (ACS) via the U.S. Census Bureau's American FactFinder (AFF) tool and were released on September 14, 2017.
Click on a state to see state and county uninsurance rates by characteristics (for example, age, race/ethnicity, and poverty level) for 2016 and comparison year 2015. Due to sample size constraints, single-year ACS estimates are available at the county level only for counties with a population greater than 65,000.
Click here to view uninsurance estimates for the United States.
Click here to view uninsurance estimates for Puerto Rico and its municipios
Note: These tables present uninsured rates, which indicate the share of the population that is uninsured. For example, a 10 percent uninsured rate for adult women indicates that 10 percent of all adult women are uninsured.
Additional Estimates (50-State Comparisons)
Maps & Tables of Private, Public, & Uninsured Change from 2015 to 2016
- Private Coverage Rates by State, Change from 2015 to 2016, for All People
- Public Coverage Rates by State, Change from 2015 to 2016, for All People
- Uninsurance Rates by State, Change from 2015 to 2016, for All People
About the ACS
The ACS is a household survey that began in 2005 and produces annually updated data on a variety of population characteristics, including health insurance coverage. In total, the ACS surveys approximately three million US households each year. An important feature of the ACS is that it includes a large enough sample for state‐level and sub‐state estimates.
The ACS began asking survey respondents about health insurance coverage during the 2008 calendar year. Specifically, the survey asks respondents about current coverage for each person in the respondent’s household. A person is categorized as “insured” if he or she has coverage at the point in time at which the survey is administered.
Why Aren’t Estimates Provided for All Counties?
Due to sample size constraints, single-year ACS estimates are available at the county level only for counties with a population greater than 65,000.
How Are these Estimates Different from the Estimates that SHADAC Publishes Using Census Bureau Micro-Data Files?
Two definitions used by the Census Bureau to generate the tabulations above differ from those that SHADAC uses to generate tabulations for State Health Compare. The definitional differences are as follows:
Family
- The Census Bureau defines a family as all related people in a household.
- SHADAC defines a family using a measure called the “Health Insurance Unit” (HIU), which includes all individuals who would likely be considered a family unit in determining eligibility for either private or public coverage.
- To learn more about the HIU, see SHADAC Brief #27, “Defining Family for Studies of Health Insurance Coverage.”
Family Income
- The Census Bureau determines family income as a percentage of the Federal Poverty Level (FPL), which is a definition of poverty used primarily for statistical purposes. For example, FPL is used to estimate the number of Americans living in poverty each year.
- SHADAC determines family income as a percentage of the U.S. Department of Health and Human Services’ Federal Poverty Guidelines (FPG), which is a measure used for administrative purposes. For example, FPG is used to determine eligibility for federal programs such as Medicaid and the Supplemental Nutrition Assistance Program (SNAP).
- To learn more about the difference between FPL and FPG, click here.

