 VISIT STATE HEALTH COMPARE
VISIT STATE HEALTH COMPARE
Publication



Health Care Reform: The Impact of Federal Health Care Reform in Minnesota
Prior to the passage of the Affordable Care Act (ACA) in 2010, Minnesota's health insurance market was, for the most part, relatively high-functioning across indicators of health insurnace access and quality of care, although the state faced common challenges in the area of health care costs. This brief, by SHADAC deputy director Elizabeth Lukanen, considers Minnesota's health insurance market before and after the passage of the ACA as well as the outlook for the state's market given the current policy environment.

Blog & News

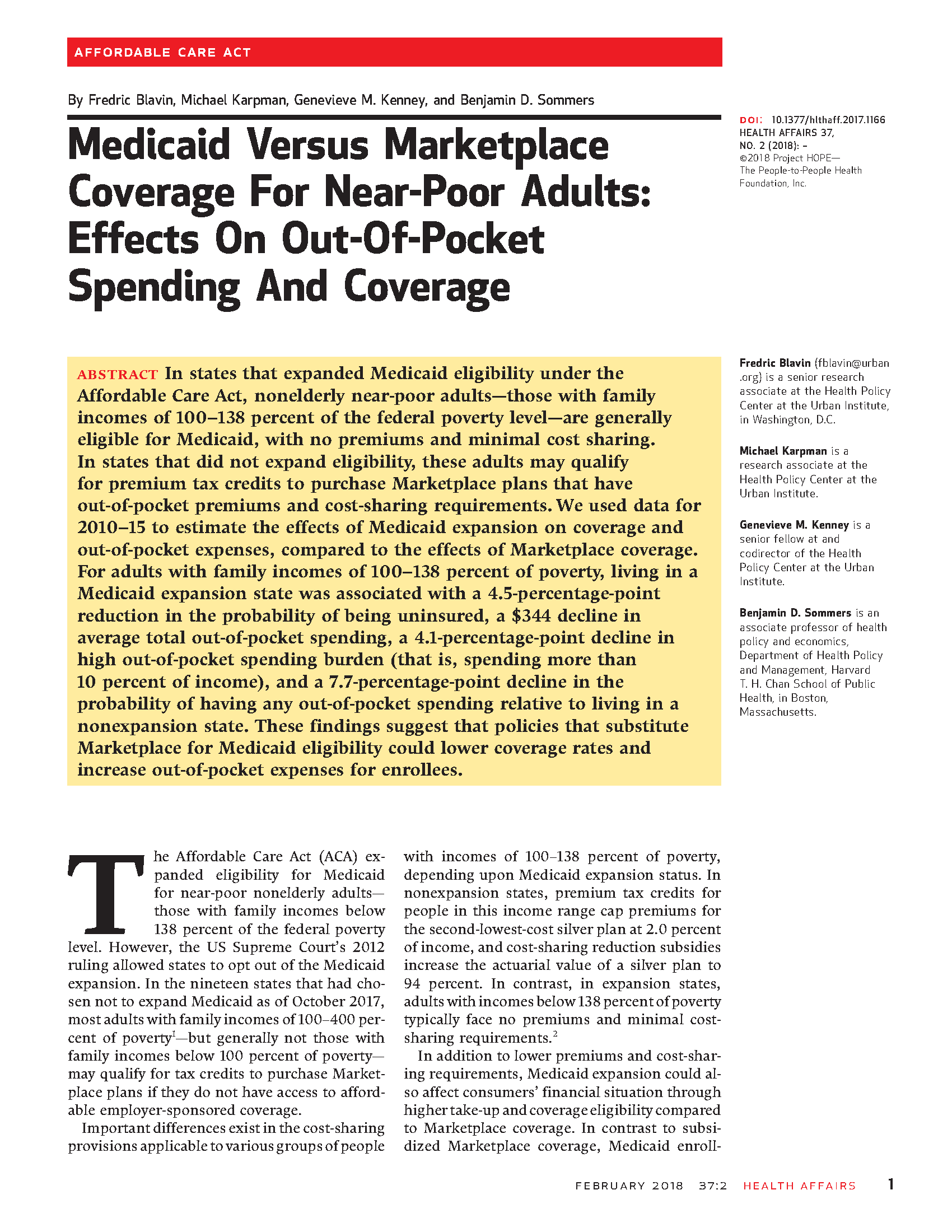
SHARE Results from Fred Blavin in Health Affairs: Among Near-Poor Adults, Access to Medicaid Reduced Out-of-Pocket Spending and Uninsurance
May 15, 2018:According to an article released today in Health Affairs, adults with incomes between 100 and 138 percent of the federal poverty level (FPL)—i.e., “near-poor” adults—saw lower out-of-pocket (OOP) costs and a reduced likelihood of being uninsured in states that expanded Medicaid than in non-expansion states.
Overview: Access to Medicaid among Near-Poor Adults
The analysis, which is based on a SHARE-funded study led by Dr. Fred Blavin (Urban Institute), used 2010 to 2015 data from the Current Population Survey (CPS) and the American Community Survey (ACS) along with state Medicaid expansion decisions as a natural experiment to estimate the impact of access to Medicaid on OOP health expenses and health insurance coverage, compared with access to subsidized Marketplace coverage. In states that chose not to expand Medicaid, near-poor adults may qualify for tax credits to purchase Marketplace plans that involve OOP premiums and cost-sharing; in expansion states, this population would generally face no premiums and minimal cost-sharing if they enrolled in Medicaid instead.
Key Findings: Out-of-Pocket Spending
Using OOP spending information from the CPS, Dr. Blavin and his co-authors found that Medicaid expansion, relative to Marketplace access, was associated with a $344 (33.9%) reduction in average total OOP spending, a $125 (23.0%) reduction in average OOP premium spending, and a $218 (46.4%) reduction in average OOP cost-sharing spending from 2010-2013 (before Medicaid expansion) to 2014-2015 (after Medicaid expansion). These decreases in average OOP spending were primarily driven by declines in the probability of having any OOP spending.
The $344 reduction in average total OOP spending from Medicaid expansion corresponds to 2 percent of annual income for adults in the 100 to 138 percent FPL range, and this is consistent with the amount that near-poor individuals would have to pay out-of-pocket for a Marketplace plan in a states that chose not to expand Medicaid. The authors note, however, that the impact of expansion for those who newly enrolled in Medicaid is likely to be higher, especially for those who had high OOP expenses prior to the ACA—e.g., high-cost uninsured adults and those with expensive employer plans.
| Related Resource: Webinar Recording and Slides | |
|---|---|
|
Dr. Blavin presented findings from this analysis during a SHARE webinar on December 5, 2017. The recording and transcript of this event, along with the presentation slides, are now available online. |
|
| Click here to access these materials. |
Key Findings: Coverage
Using coverage information from the ACS, the authors found that Medicaid expansion reduced the probability of being uninsured among near-poor adults by 4.5 percentage points between 2010-2013 and 2014-2015, compared to non-expansion states. This impact was driven by significant increases in Medicaid coverage that were partially offset by declines in ESI and direct purchase coverage.
According to the authors, these findings imply that more restrictive eligibility and enrollment policies, combined with higher premiums for Marketplace coverage relative to Medicaid, were associated with lower take-up rates among near-poor adults.
Read the full Health Affairs article.
Blog & News

The Children's Health Insurance Program: A Minnesota Perspective
January 22, 2018:Congress has still not fully reauthorized the Children’s Health Insurance Program (CHIP), and states are working to figure out how to keep their kids covered. CHIP provides essential coverage for millions of our nation’s poorest children and should not be used as a bargaining tool in federal budget negotiations. It’s time to put politics aside and reauthorize this program that is vital for vulnerable children and that both sides ofthe aisle claim to support.
Minnesota: A Pioneer in Covering Kids
Minnesota, as a national leader in health care, has a long history of providing coverage for its children--well before the passage of the federal CHIP program. As far back as 1987, Minnesota provided coverage to low-income children who were just above the income level to qualify for Medicaid, and we paid for it with state funds alone. The program initially covered physician services for children under age six and low-income pregnant women who were not Medicaid-eligible. The state financed the program through an annual fee of $35 for pregnant women and $25 for children, and a one-cent tax on cigarette packs.
In 1991, Minnesota's public coverage for kids was expanded to all children under age 18, and in 1992, Governor Carlson passed comprehensive health reform legislation, the HealthRight Act, with broad bipartisan support. Renamed MinnesotaCare, the state's public coverage program provided subsidized health insurance for working families with incomes just above Medicaid eligibility levels (up to 275% of the Federal Poverty Level) who not eligible for employer-sponsored insurance. The program continued to be funded with state-only dollars, and the legislation behind it included earmarked funding from a new 2% provider tax, a 1% health insurance premium tax, as well as a five-cent increase in the cigarette tax.
Early analyses of the impact of MinnesotaCare found that between 1990 and 1995 the proportion of uninsured children (uninsured for 12 months or longer) in Minnesota decreased from 5.2% to 3.1%. This change translated to an increase in access to care for kids and a reduction in the amount of free care given by medical providers to the uninsured.
CHIP's Evolving Role in Minnesota and the Nation
Minnesota and other states that had similarly funded their own safety net programs were thrilled when CHIP passed in 1997. Modeled in part on the Minnesota program, CHIP targeted families just above the eligibility level for Medicaid and provided needed support to low-income working families. In its early years, CHIP funded very few of Minnesota’s low-income children, as the program was targeted to states with larger numbers of uninsured children; in fact, a report from 2000 showed only 8 children in Minnesota covered by CHIP. However, Minnesota leveraged CHIP funding over time, and today Minnesota uses its CHIP dollars to support coverage for 127,000 children and pregnant women. Nationwide, the program is now well-established and covers close to 9 million children.
The Uncertain Future of CHIP Puts the Most Vulnerable at Risk
Minnesota’s goal has always been to get and keep children and their families insured. We know that providing health insurance coverage enhances children’s school performance, increases parents’ work attendance, improves and sustains high immunization rates, and advances the health and economic future of children as they age into adulthood. Most of all, coverage assures that all have an opportunity to pursue their goals and aspirations in life.
Both the delay in the CHIP reauthorization and the real potential for no future funding affects the most vulnerable: poor children. It’s hard to believe, but close to one in every four children in this country lives in poverty. For African American children, the rate is over 40%.
States Employing Stopgap Measures
With the end of CHIP’s authorization on September 30th, states have been able to apply for emergency funding to keep their programs going. Oregon and Minnesota have both pledged to make up what they hope is a temporary funding gap with state dollars, but it puts their finances in jeopardy — Minnesota’s latest budget projection released in early December includes a $188 million shortfall if CHIP is not reauthorized. Meanwhile, other states will need to shut down new enrollment and start notifying families of potential loss of coverage.
In the meantime, the stress to families of not knowing if coverage will continue and for how long, is real. States are scrambling to keep kids covered — making tremendous efforts to find alternative funding, notifying families of the potential phase out of the program, and placing limits on new enrollment in anticipation of a lack of funding.
Funding CHIP: A No-Brainer and the Right Thing to Do
Lynn A. Blewett, PhD, MPA, is Professor of Health Policy at the University of Minnesota, School of Public Health
Publication
Data Resources for Conducting Health Services and Policy Research

Blewett, LA, Call, KT, Turner J, & Hest, R. (2017). "Data Resources for Conducting Health Services and Policy Research." Annual Review of Public Health 39: 437-452. doi: 10.1146/annurev-publhealth-040617-013544
This article examines six federal household surveys that provide data inputs for monitoring the health and health care of the U.S. population and that are important for conducting helath services policy research: American Community Survey, Current Population Survey, National Health Interview Survey, Behavioral Risk Factor Surveillance System, Medical Expenditure Panel Survey, and Survey of Income and Program Participation.
Blog & News
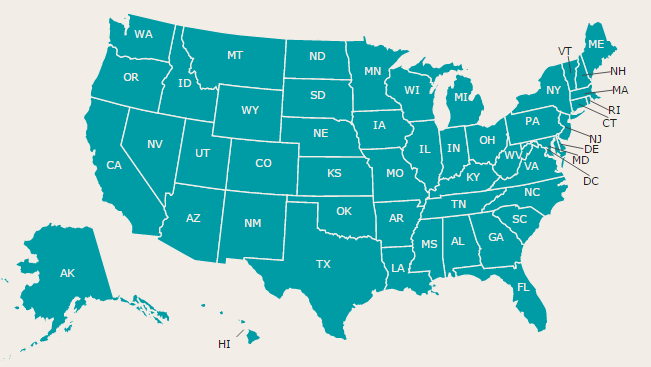
Updated Health Insurance Coverage Estimates Available for All U.S. Counties
December 12, 2017:SHADAC tables of state and county uninsurance estimates for 2012 to 2016 are now available via clickable map. Users can click a state to access a table of 5-year uninsurance estimates for the state and all counties using data from the American Community Survey (ACS).
 Data Background
Data Background
The 5-year ACS is created by pooling together five years of ACS data to produce estimates for areas and subgroups with smaller populations. With the 5-year pooled data, estimates are available even for counties with a population below 65,000 (for which estimates are not available with just a single year of ACS data).
Related Resource
SHADAC’s State Profiles have been updated to include these 5-year estimates.

