Blog & News





Now Available on State Health Compare: Eleven Updated Measures and One Brand New Measure
December 3, 2019:Estimates for measures from a variety of categories (Health Outcomes, Health Behaviors, Access to Care, Cost of Care, and Social and Economic Factors, etc.) have now been updated on SHADAC’s State Health Compare web tool. All measures now contain data for 2018, the most recent year available. State Health Compare has also added a brand new measure, Adult E-Cigarette Use.
Updated Measures Include:
Income Inequality
Using the Gini coefficient (a summary of the dispersion of income across the entire income distribution), this measure gauges disparities in income in each state on a scale from 0 to 1, with higher values indicating greater inequality and lower values indicating the opposite. Estimates for all states are now available from 2006 through 2018.
Sales of Opioid Painkillers
This measure captures the rate of legal prescription opioid painkiller sales in kilograms per 100,000 people per year for both hydrocodone and oxycodone—the most common types of prescription opioids. Data is now available for all states from 2000 through 2018.
Adults Who Forgo Needed Medical Care*
The measure indicates the percent of adults (18+) in each state who could not get needed medical care due to cost. Breakdowns by education level and race/ethnicity are available for all states from 2005 through 2010 and 2011 through 2018.
Adults With No Personal Doctor*
This measure denotes the percent of adults without a personal doctor and is now available for all states from 2005 through 2010 and 2011 through 2018. Breakdowns by education level and race/ethnicity are also available.
Adult Cancer Screenings*
The measure is an indication of the percent of adults who have received recommended cancer screenings (e.g., colorectal screenings, mammograms, pap smears, etc.) in the past year, and is now available for all states from 2005 through 2010 and 2011 through 2018.
Chronic Disease Prevalence*
This measure captures the percent of adults who reported having one or more common chronic conditions such as diabetes, cardiovascular disease, heart attack, stroke, and asthma, in each state. Estimates are now available for all states from 2005 through 2010 and 2011 through 2018.
Activities Limited due to Health Difficulty*
This measure reports the average number of days (in the last 30 days) for which an adult indicates limited activity due to mental or physical health difficulties. It is now available for all states from 2005 through 2010 and 2011 through 2018.
Adult Obesity*
The measure is an indication of the prevalence of obesity, defined as a Body Mass Index (BMI) > 30, among the adult population 18 years of age and over. It is now available for all states from 2005 through 2010 and 2011 through 2018.
Adult Binge Drinking*
This measure indicates the percent of adults who, on one occasion, have consumed at least four drinks (women) or five (men) or more in the past 30 days. Now available for all states from 2005 through 2010 and 2011 through 2018, the measure includes breakdowns by education level and race/ethnicity.
Adult Smoking*
This measure indicates the percent of adults over 18 years of age who have smoked 100 or more cigarettes in their lifetime, and who currently smoke some days or every day. It is now available for all states from 2005 through 2010, and 2011 through 2018.
Adult E-Cigarette Use (Newly available measure on State Health Compare)
This measure indicates the percent of the adult population (18 years of age and over) who currently use e-cigarette some days or every day. It is now available for all states from 2016 through 2017 and for most states for 2018. Breakdowns are available by education level and race/ethnicity.
Data Sources
The State Health Compare estimates for income inequality come from the American Community Survey (ACS); the sales of opioid painkillers comes from the U.S. DEA’s Automated Reports Consolidated Ordering System Retail Drug Summary Reports; and the measures of chronic disease prevalence, activities limited due to health difficulty, and the adults who forgo needed medical care, adults with no personal doctor, and adult cancer screenings, obesity, binge drinking, smoking, and e-cigarette use measures all come from the Behavior Risk Factor Surveillance System (BRFSS).
Notes
All measures marked with an “*”: This indicates a break in series due to the BRFSS implementing cell phone sampling and an advanced weighting method in 2011.
Blog & News

Minnesota's Growing and Evolving Opioid Crisis
October 28, 2019: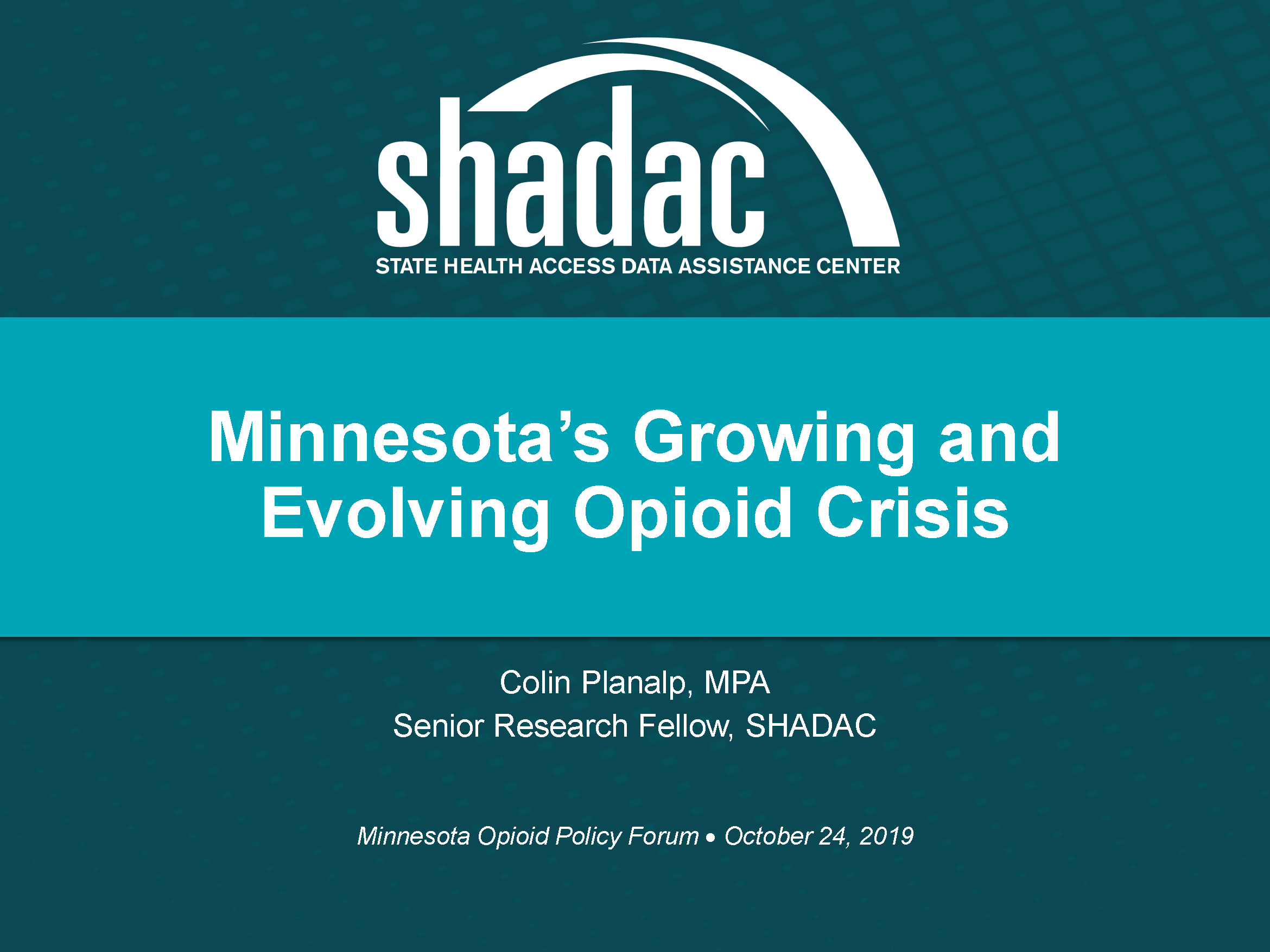 On Thursday, October 24, SHADAC Senior Research Fellow Colin Planalp presented a data-focused look at Minnesota’s opioid crisis during the University of Minnesota’s Medical Industry Leadership Institute “Combating Minnesota’s Opioid Epidemic” policy forum. Colin shared the stage with experts in a variety of arenas and policy levels including state and federal legislators and local stakeholders, as well as health insurers, health care providers, and payers, for this one-day event aimed at learning from and building on current efforts to successfully combat the opioid epidemic.
On Thursday, October 24, SHADAC Senior Research Fellow Colin Planalp presented a data-focused look at Minnesota’s opioid crisis during the University of Minnesota’s Medical Industry Leadership Institute “Combating Minnesota’s Opioid Epidemic” policy forum. Colin shared the stage with experts in a variety of arenas and policy levels including state and federal legislators and local stakeholders, as well as health insurers, health care providers, and payers, for this one-day event aimed at learning from and building on current efforts to successfully combat the opioid epidemic.
Across the states, the opioid crisis varies widely—both in the range of opioid death rates and in differences regarding the types of opioids that cause the most deaths (prescription opioid painkillers, heroin, synthetic opioids, etc.). For example, deaths from synthetic opioids, such as fentanyl, ranged from a low of 1.2 per 100,000 people in Kansas and Texas in 2017 to a high of 37.4 deaths per 100,000 people in West Virginia—a difference of more than 30 times (Figure 1).
Figure 1. State Synthetic Opioid Death Rates per 100,000 People, 2017

In 2017, Minnesota had one of the lowest overdose death rates among all 50 states for synthetic opioids, at 3.5 deaths per 100,000 people, which was also significantly lower than the U.S. rate of 9.0 deaths per 100,000 people (Figure 2). Minnesota’s death rates from heroin and prescription opioid painkillers also were significantly lower than the U.S. rate in 2017 (not shown).
Figure 2. State vs. National Synthetic Opioid Death Rates per 100,000 People, 2017
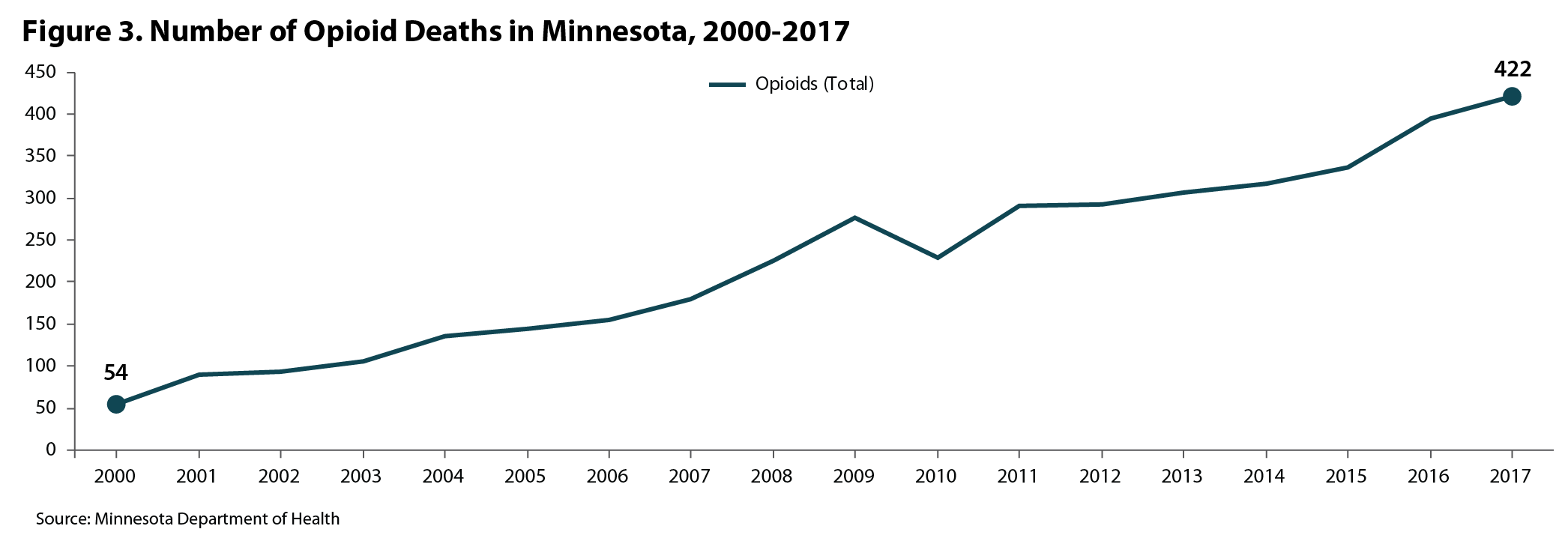
Although Minnesota has not been hit as severely as many other states, it would be wrong to assume the opioid crisis isn’t a problem in the state. Since 2000, the number of deaths attributed to opioid overdoses has increased nearly seven times, from 54 to 422 in 2017 (Figure 3).
Figure 3. Number of Opioid Overdose Deaths in Minnesota, 2000-2017
Despite common misconceptions about the kinds of communities affected by the opioid crisis—either that it’s only an urban problem or only a rural problem—data on opioid overdose deaths show that Minnesota’s opioid crisis isn’t limited geographically. Since 2000, opioid deaths have increased substantially in both the seven-county Twin Cities region and outside the Twin Cities in greater Minnesota. In the Twin Cities Metro, opioid deaths increased about 5.5 times, from 43 in 2000 to 280 in 2017; and they grew almost 12 times in greater Minnesota, from 11 to 142 deaths during the same time period (not shown).
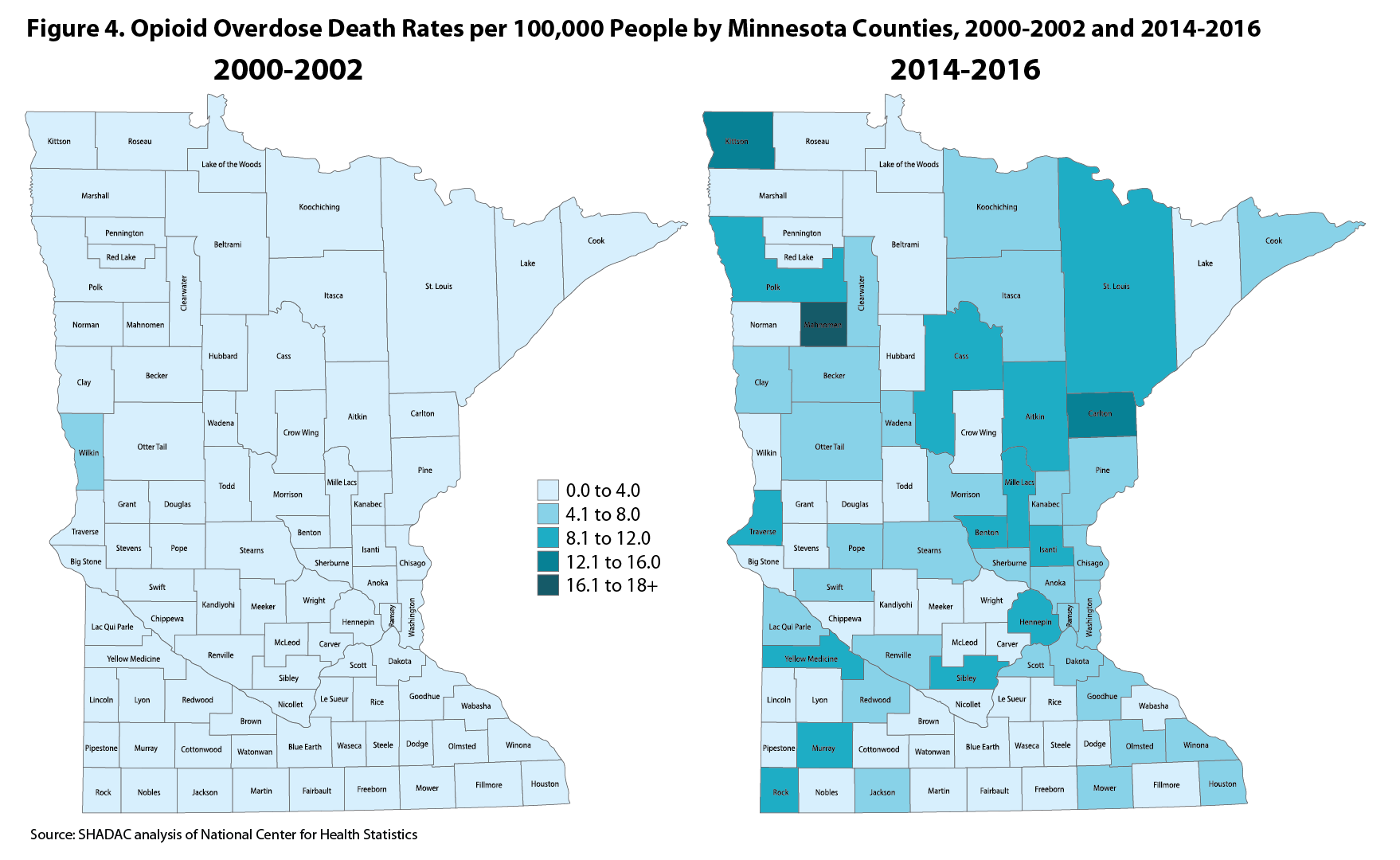
A map of Minnesota counties paints a similar picture. During the three years from 2000-2002, only one of Minnesota’s 87 counties had an opioid death rate of more than 4.0 deaths per 100,000 people, but during the period from 2014-2016, most of the state’s counties (46 of 87) had an opioid death rate of more than 4.0 deaths per 100,000 people (Figure 4).
Figure 4. Opioid Overdose Death Rates per 100,000 People by Minnesota Counties, 2000-2002 and 2014-2016
Preliminary data on opioid overdose deaths published by the Minnesota Department of Health suggest that Minnesota may be turning a corner. If the preliminary data regarding overdose deaths hold accurate in the final count, Minnesota will experience a drop in total opioid overdose deaths in 2018 compared with 2017—only the second time that has happened since 2000. Despite that encouraging sign, however, the data show continued reasons for serious concern:
- First, even with a decline in 2018, the provisional data showing more than 300 opioid overdose deaths last year still represents a near-historic high.
- Second, while the total number of opioid overdose deaths may have declined, deaths from certain types of opioids continued to climb, with nearly 200 deaths resulting from synthetic opioids recorded in 2018.
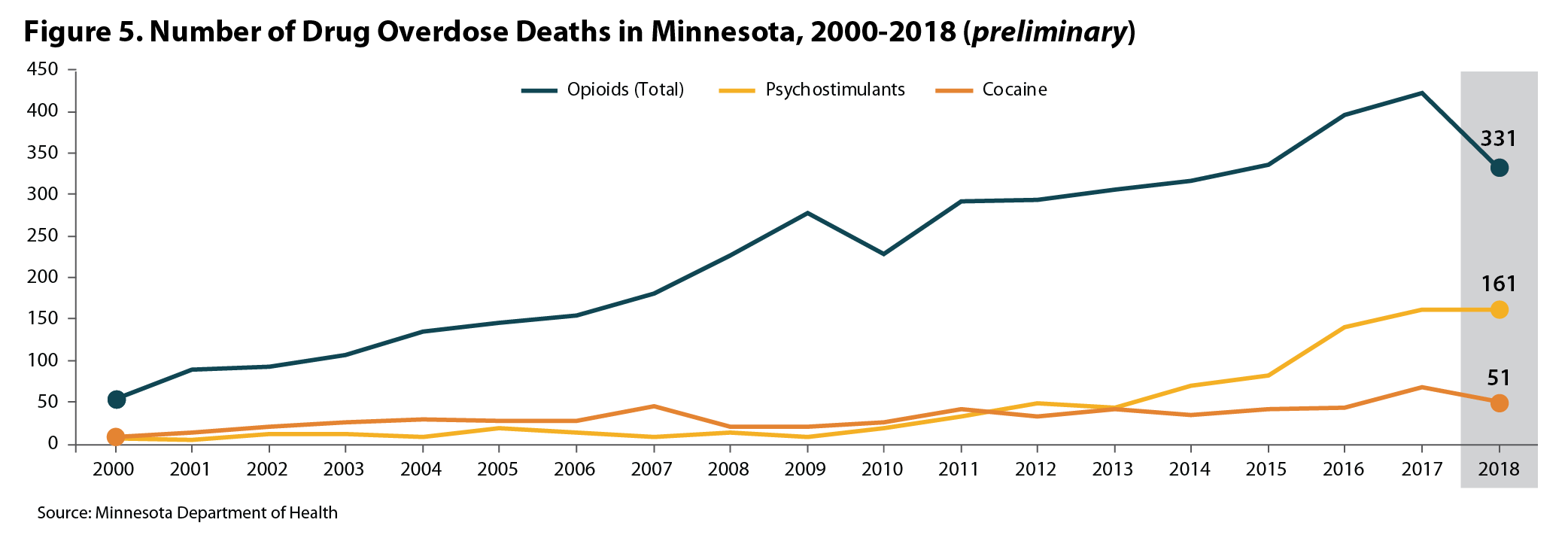
- Third, drug overdose death data from Minnesota show signs that the opioid crisis may be spreading to non-opioid substances, such as methamphetamine and cocaine—a trend consistent with data for the U.S. and for other states. Minnesota’s 2017 and provisional 2018 data show cocaine and psychostimulant (e.g., methamphetamine) deaths at or near historic highs (Figure 5).
Figure 5. Number of Opioid Overdose Deaths in Minnesota, 2000-2018 (preliminary)