 VISIT STATE HEALTH COMPARE
VISIT STATE HEALTH COMPARE
Blog & News





Minnesota Community and Uninsured Profile Updated to Include 2022 American Community Survey Estimates
August 12, 2024:|
|
 |
 |
- Provide information on Minnesota uninsured people and populations
- Assist policymakers in developing & evaluating enrollment and outreach strategies
- Understand uninsured community and population characteristics in Minnesota
- Create a tool that can be used to understand and evaluate equity work, inform strategic planning, assess community needs, and support grant writing for related and relevant programs
- How to Use - an overview on using the uninsured profile to both identify and gather information communities of interest
- Community and Uninsured Profile - the profile itself with breakdowns at the county, MNsure rating area, ZIP code, economic development region, and state levels
- ZIP Code Uninsured Rates - includes all reported Census-defined ZIP Codes, regions, and counties in Minnesota along with both the number and percent of uninsured within those communities

Interactive Map
Learn more about the profile and download the data here, where you can also find out how to use the profile, including a tutorial video.
Want to learn more about how we made this profile? Curious about its applications? Contact us here – we are always happy to discuss.
Related Products:
Blog & News

2020 Public Use Microdata Area (PUMA) Updates in the 2022 American Community Survey
March 26, 2024:A Public Use Microdata Area (PUMA) is a type of geographic unit created for statistical purposes. PUMAs represent geographic areas with a population size of 100,000–200,000 within a state (PUMAs cannot cross state lines). PUMAs are the smallest level of geography available in American Community Survey (ACS) microdata. They are designed to protect respondent confidentiality while simultaneously allowing analysts to produce estimates for small geographic areas.
Every ten years, the decennial census results are used to redefine ACS PUMA boundaries to account for shifts in population and continue to maintain respondent confidentiality. This process is intended to yield geographic definitions that are meaningful to many stakeholders.
Most recently, new PUMAs were created based on the 2020 Census; these 2020 PUMAs were implemented in the ACS starting in the 2022 data year. Although Public Use Microdata Area components remain consistent to the extent possible, they are updated based on census results and revised criteria. Therefore, they are not directly comparable with PUMAs from any previous ACS data years. For example, the 2020 PUMAs used in the 2022 data year are distinct from the 2010 PUMAs, which were used in the 2012–2021 ACS data years.
The 2020 PUMAs were created based on definitions that include two substantive changes relative to the 2010 PUMAs:
1) An increase in the minimum population threshold for the minimum size of partial counties from 2,400 to 10,000. Increasing the population minimum for a PUMA-county part aims to further protect the confidentiality of respondents. However, exceptions are allowed on a case-by-case basis in order to maintain the stability of PUMA definitions (that were based on the previous minimum of 2,400) and due to unique geography.
2) Allowing noncontiguous geographic areas. Allowing PUMAs to include noncontiguous geographic areas aims to avoid unnecessarily splitting up demographic groups in order to provide more meaningful data. This change is not intended to create highly fragmented PUMAs.
Other than the two changes listed above, PUMA criteria remained consistent, such as treating 100,000 as a strict minimum population size for PUMAs. The maximum population size for PUMAs can exceed a population of 200,000 in certain instances due to expected population declines or geographic constraints.
Generally, counties and census tracts are the building block geographies for PUMAs. This maximizes the stability of PUMA boundaries and therefore reduces disclosure risks. Counties may be combined or split as needed, depending on population size. Additionally, PUMAs are designed to avoid unnecessarily splitting metropolitan areas, minor civil divisions (MCDs) with a functional government, and areas of American Indian/Alaska Native (AIAN) and Native Hawaiian people. Carlton County in Minnesota, for example, illustrates that splitting a county was necessary to avoid splitting Fond du Lac reservation into multiple PUMAs (U.S. Census Bureau, 2022).
Figure 1: Minnesota PUMA 00400 Includes Fond du Lac Reservation in Its Entirety

Note: Minnesota PUMA 00400 featuring Fond Du Lac Reservation in its entirety. Reprinted from Final Criteria for Public Use Microdata Areas for the 2020 Census and the American Community Survey from https://www2.census.gov/geo/pdfs/reference/puma2020/2020PUMA_FinalCriteria.pdf.
Due to periodic changes in Public Use Microdata Area boundaries, states as a whole are the most granular geographic variable in the ACS microdata that can be compared consistently across all years. However, IPUMS USA offers harmonized geographic variables that greatly expand the options for analyzing ACS data across both time and geography. These variables are less granular than PUMAs, but more granular than states. For example, CONSPUMA and CPUMA0010 combine ACS PUMAs to create consistent geographies that can be compared across multiple decades of PUMA definitions; these have not yet been updated to include the new 2020 PUMAs. Currently, CITY, COUNTYFIP, and MET2013 allows users to compare cities, counties, and metropolitan areas, respectively, over years 2005-2022.
IPUMS USA also provides in-depth geographic resources for ACS data users, including interactive maps of the 2010 and 2020 PUMAs. For example, below is a map of the Twin Cities metropolitan area, Minnesota, showing 2020 PUMAs in blue and 2010 PUMAs in orange (IPUMS USA, 2020). This map illustrates that the updated PUMA criteria resulted in changes to PUMA boundaries in urban areas and some aggregation of PUMAs in more rural areas.
Figure 2: IPUMS USA Map of Twin Cities Metropolitan Area, Minnesota 2010 and 2020 PUMAs
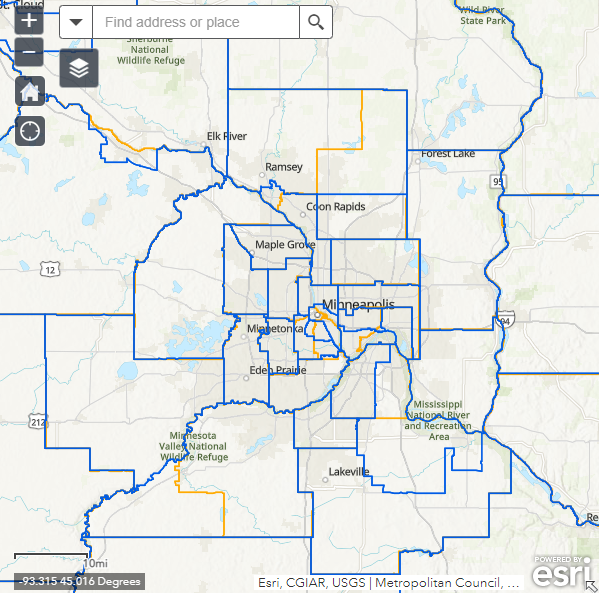
Note: IPUMS USA Map of Twin Cities Metropolitan Area, Minnesota 2010 and 2020 PUMAs. Reprinted from 2020 PUMA DEFINITIONS: WEB MAP OF 2010 AND 2020 PUMAS from IPUMS USA, https://usa.ipums.org/usa/volii/pumas20.shtml.
Looking for other data and information from the American Community Survey? Learn more with the following SHADAC products:
2022 ACS Tables: State and County Uninsured Rates
American Indian/Alaska Native (AIAN) and Native Hawaiian and Other Pacific Islander (NHPI) data added to State Health Compare ACS estimates
Explore the Data on State Health Compare
Sources:
U.S. Census Bureau. (2022, July 25). Final Criteria for Public Use Microdata Areas for the 2020 Census and the American Community Survey. https://www2.census.gov/geo/pdfs/reference/puma2020/2020PUMA_FinalCriteria.pdf
IPUMS USA (2020). 2020 PUMA Definitions: Web Map of 2010 and 2020 PUMAs. https://usa.ipums.org/usa/volii/pumas20.shtml.
Publication
Using Enrollment Records to Evaluate Self-Reports of Monthly Coverage in the Redesigned Current Population Survey Health Insurance Module
This journal article was originally published on January 23, 2024, in Health Services Research.
Introduction

This article, authored by SHADAC Investigator Dr. Kathleen T. Call alongside colleagues from the U.S. Census Bureau Angela R. Fertig and Joanne Pascale, explores the veracity of self-reports of month-level health insurance coverage in the Current Population Survey Annual Social and Economic Supplement (CPS ASEC).
The CHIME (Comparing Health Insurance Measurement Error) study used health insurance enrollment records from a large regional Midwest insurer as the sample for primary data collection in spring of 2015. In this study, a sample of individuals enrolled in a range of public and private coverage types (including Medicaid and marketplace) was administered the CPS health insurance module, which included questions about month-level coverage, by type, over a 17–18-month time span. Survey data was then matched to enrollment records covering that same time frame, and concordance between the records and self-reports was assessed.
Principal Findings
For 91% of the overall sample, coverage status and type were reported accurately for at least 75% of observed months.
Among those who were continuously covered throughout the 17–18 month observation period (64% of the overall sample), that level of reporting accuracy was observed for 94% of the sample. For those who had censored spells (34% of the overall sample), the figure was 87%. Among those with gaps and/or changes according to the records (2% of the overall sample), for 82% of the group at least 75% of months were reported accurately.
These findings suggest that reporting accuracy of month-level coverage is high - thus, this survey could become a new data source for studying overall dynamics of health insurance coverage, namely the Medicaid unwinding.
To read the full article, visit this link.
Learn more about:
Publication
Did Disparities in Access Worsen During the Pandemic? (CHCF Brief)
The following content is cross-posted from California Health Care Foundation
Author: Lacey Hartman, SHADAC
Previous research has shown that Medi-Cal enrollees fare worse in accessing health care than Californians with employer coverage. A key question is whether and how access to care shifted during the pandemic for the two groups. For example, did existing differences in access worsen or improve? Have new access challenges emerged for those with Medi-Cal, compared to those with employer coverage?
To answer these questions, authors of a new CHCF brief compared data from the 2017–18 and 2020–21 California Health Interview Survey (CHIS). Separate analyses were done for adults and children.

Key findings include:
- Data show that the pandemic did not widen differences in access to care for people with Medi-Cal coverage compared to those with employer coverage. This held true for both adults and children.
- Rather, among adults, there was some narrowing of differences on select measures. However, this is not a positive development, as it appears to have been caused by worsening access to care for adults with employer-sponsored insurance coverage during the pandemic rather than improvements for adults with Medi-Cal.
Authors note that a key issue going forward is how the end of the federal Medicaid continuous coverage requirement will impact access to care among Californians.
Blog & News

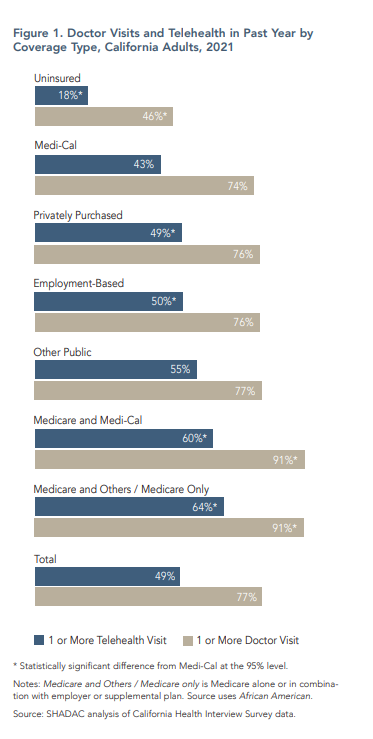
Telehealth Use and Experiences Among California Adults (CHCF Brief)
September 12, 2023:The following content is cross-posted from the California Health Care Foundation (CHCF).
Author: Lacey Hartman, Senior Research Fellow, State Health Access Data Assistance Center
California’s Medi-Cal program is leveraging telehealth to meet patient needs. Many of the telehealth coverage and reimbursement flexibilities enacted during the pandemic were made permanent in 2022, including payment parity for services provided in person or by telehealth. With the end of the public health emergency, there are important questions about how telehealth is being used to meet patients’ needs and which flexibilities should remain in place over the long term.
This CHCF issue brief authored by SHADAC's Senior Research Fellow Lacey Hartman, uses data from the 2021 California Health Interview Survey (CHIS) to explore how telehealth use varies across subpopulations of adults in the state and reports how people rate their telehealth experience compared to in-person care. The brief concludes with a discussion of potential policy implications of the findings, and areas for future data collection and research.
Key findings:
- Telehealth use varies by coverage type, race/ethnicity, and language
- People on Medi-Cal use less telehealth
- Less English proficiency is associated with less telehealth use
- Black Californians are more likely to use telehealth
- Most Californians who use telehealth like it as much as or better than in-person care
Our findings suggest that telehealth use follows the variation in the use of doctor visits overall. People who report more doctor visits also tend to use more telehealth, and people less likely to go to the doctor also tend to use less telehealth, with some important exceptions, including by coverage type, race/ethnicity, and language. Often, telehealth does not exacerbate overall disparities in health care access. However, while many people report that telehealth improves access to care, more telehealth use did not eliminate access to care disparities at the population level during the pandemic. The likely cause is the persistence of structural barriers, such as limited provider availability, even as telehealth use has grown.

