 VISIT STATE HEALTH COMPARE
VISIT STATE HEALTH COMPARE
Blog & News





Coverage During a Crisis: Insured Rate for Californians Hits Historic High in First Year of COVID-19 Pandemic (CHCF Cross Post)
September 13, 2023:The following content is cross-posted from California Health Care Foundation. It was first published on January 12, 2022.
Author: Lacey Hartman, Senior Research Fellow, SHADAC
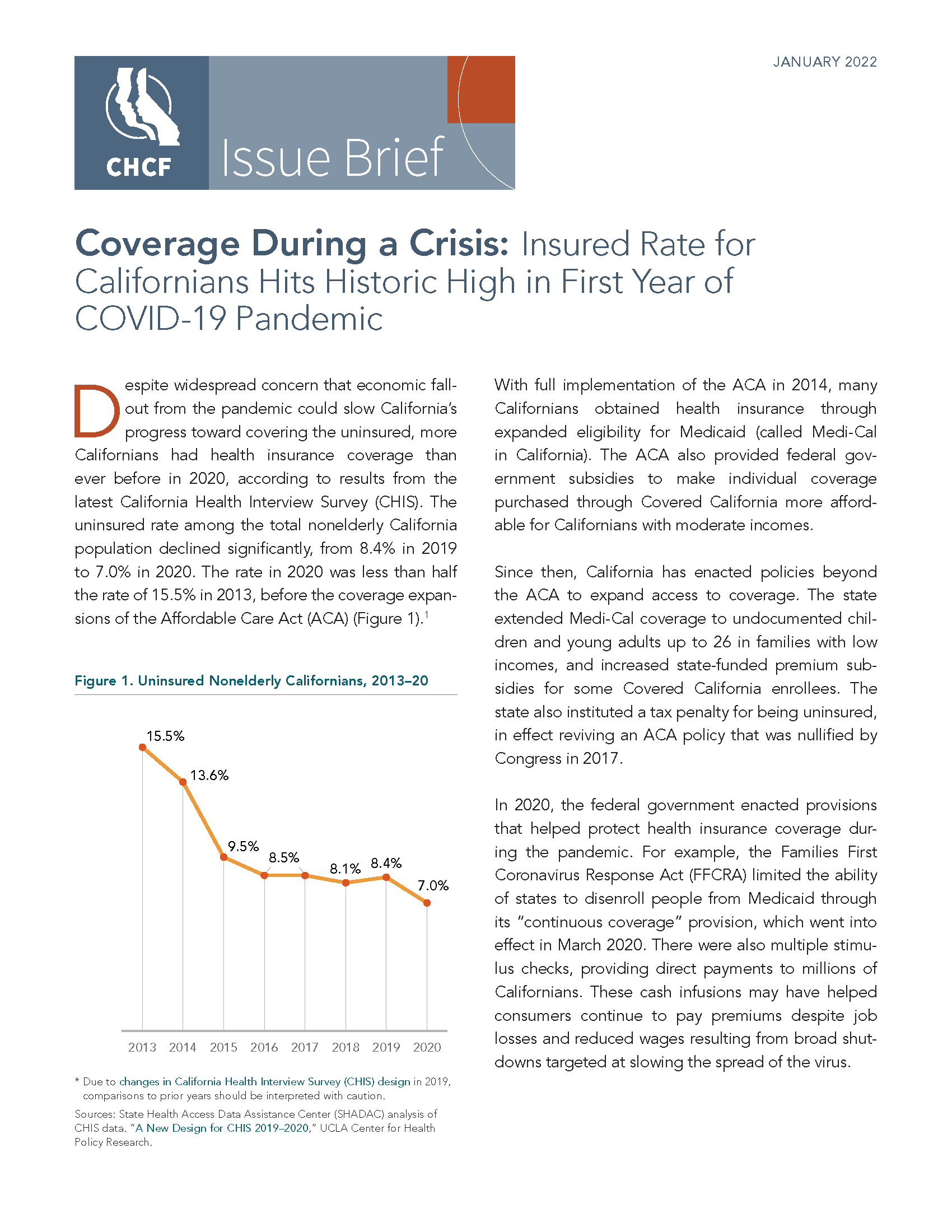
Despite widespread concern that economic fallout from the pandemic could slow California’s progress toward covering the uninsured, more Californians had health insurance coverage than ever before in 2020, according to results from the latest California Health Interview Survey (CHIS). A combination of pre-pandemic state and federal policies that expanded health insurance coverage, along with quick action by policymakers in 2020 to bolster those policies with additional crisis stopgaps, helped protect coverage for many Californians during the pandemic.
In this brief prepared for the California Health Care Foundation (CHCF), SHADAC researcher Lacey Hartman, MPP, provides data from the CHIS about the coverage landscape in California in 2020, highlighting both encouraging trends and persistent disparities that warrant attention, particularly as federal policies that protect coverage connected to the pandemic end or wind down.
Key Findings
- The uninsured rate among the nonelderly California population declined significantly, from 8.4% in 2019 to 7.0% in 2020.
- Rates of uninsured dropped across several population subgroups from 2019 to 2020.
- Californians with incomes up to 138% of the federal poverty guidelines (FPG), dropping from 12.1% to 9.6%. (These are people whose income would make them eligible for Medi-Cal, many through the Affordable Care Act [ACA] expansion of the program.)
 Californians who identify as Latinx, from 12.9% in 2019 to 10.5%.
Californians who identify as Latinx, from 12.9% in 2019 to 10.5%.- Those residing in rural areas of the state, from 9.6% to 6.4%.
- Adults age 18 to 64, from 10.8% to 9.1%.
- Employer and individual coverage held steady statewide, and increased for some groups.
- The overall statewide rate of employer coverage among the nonelderly was statistically unchanged from 58.8% in 2019 to 60.1% in 2020.
- Employer coverage increased significantly from 59.2% to 60.9% among nonelderly adults, from 62.6% to 64.9% among citizens, and from 20.5% to 24.0% among those with incomes up to 138% FPG.
- Medi-Cal coverage held steady statewide, but declined significantly among Black Californians.
- Medi-Cal coverage held steady between 2019 and 2020, covering roughly one quarter of the nonelderly population.
- Changes by subpopulation were also limited, with the notable exception that the share of Black Californians with Medi-Cal declined from 34.5% in 2019 to 24.0% in 2020, a difference that was statistically significant, and is a continuation of recent trends.
- Despite measurable progress, critical disparities in coverage persist.
- The uninsured rate among Latinx Californians remains almost three times as high as that of their White counterparts (10.5% compared to 3.8%).
- Noncitizen adults are uninsured at more than three times the rate of their citizen counterparts (18.4% compared to 5.6%).
- Californians with lower incomes are more likely to be uninsured than those with incomes above 400% FPG.
Looking Ahead
The state’s robust implementation of the Affordable Care Act and additional state policies over the years, in combination with recent state and federal policies designed to protect against coverage losses during the pandemic, has enabled the rate of coverage among Californians to rise to historic levels, even during a massive public health and economic crisis. However, there is potential for coverage expansion to slow or even reverse as policies that provided robust protection during the pandemic unwind or scale back.
Blog & News

NHIS: Early Release Estimates for January-June 2021 Show Continued Significant Changes in Public and Private Coverage across All Groups
November 22, 2021:A report of health insurance coverage estimates for the first half of 2021 (January to June) from the National Health Interview Survey (NHIS) has just been released by the National Center for Health Statistics (NCHS) as part of the NHIS Early Release Program.
Comparing the 2021 estimates to the same time period in 2020 showed broadly similar overall trends by coverage type:
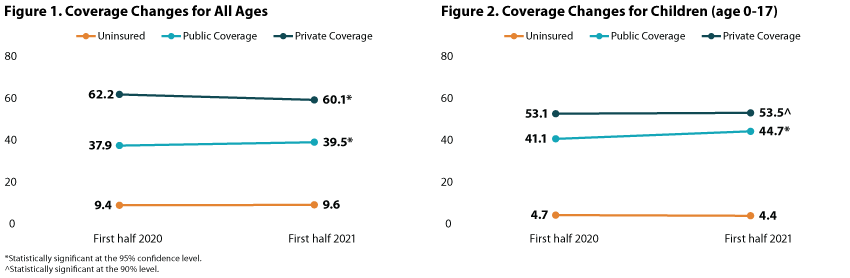
- The rate of individuals without health insurance coverage was statistically unchanged for those of all ages (9.6 percent) as well as for children age 0-17 (4.4 percent).
- The rate of individuals with public coverage increased for those of all ages to 39.5 percent from 37.9 percent, and to 44.7 percent from 41.1 percent for children age 0-17.
- The rate of individuals with private coverage decreased to 60.1 percent from 62.2 percent for those of all ages and dropped to 53.1% from 53.5% for children (age 0-17)—though this change was only statistically significant at the 90% confidence level.
Analysis of coverage trends for specific subpopulations, however, revealed larger differences among nonelderly respondents (age 0-64).
Findings by race/ethnicity
Large disparities in rates of uninsurance persisted from 2020 to 2021, with Hispanic/Latino individuals being more than twice as likely to be uninsured compared with all nonelderly individuals (23.6 percent versus 11.4 percent). Additionally, the share of nonelderly Hispanic/Latino people who were uninsured increased to 23.6 percent from 19.7 percent.
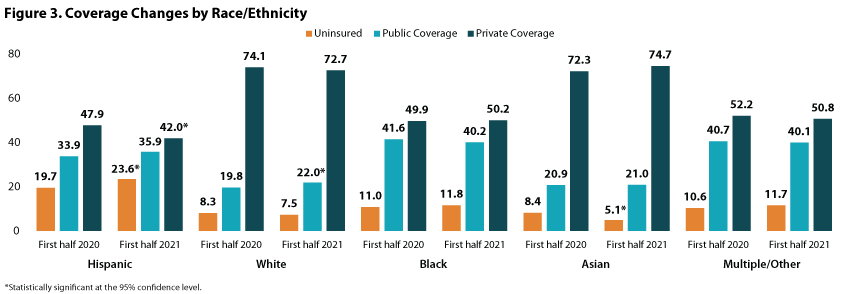
Examining uninsured rates for individuals of other races/ethnicities showed that uninsurance decreased to 5.1 percent from 8.4 percent for nonelderly Asian individuals, but was stable among White individuals, Black individuals, and persons who reported as Multiple/Other race at 7.5 percent, 11.8 percent, and 11.7 percent, respectively.
Looking at public coverage in the first half of 2021, the share of nonelderly White persons who had public coverage increased to 22.0 percent from 19.8 percent in the first half of 2020 while remaining stable among: Hispanic/Latino people (35.9 percent), Black people (40.2 percent), Asian people (21.0 percent), and those of Multiple/Other race (35.4 percent).
Conversely, the share of Hispanic/Latino nonelderly individuals with private coverage fell to 42.0percent in the first half of 2021 from 47.9 percent in the same time period of 2020. Rates of private coverage, however, were stable among White individuals (72.7 percent), Black individuals (50.2 percent), Asian individuals (74.7 percent), and individuals of Multiple/Other race (50.8 percent).
Findings by Medicaid Expansion status
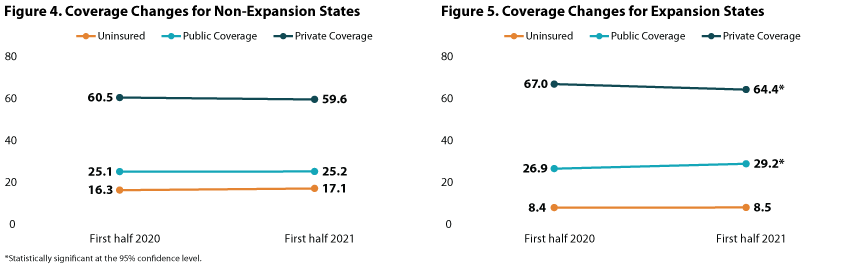
For January-June 2021, nonelderly individuals (age 0-64) living in non-expansion states were more than twice as likely to be uninsured than those living in expansion states at 17.1 percent vs. 8.5 percent—though these rates were both stable when compared with rates from January-June 2020.
In expansion states, rates of public coverage increased to 29.2 percent (from 26.9 percent) while rates of private coverage conversely decreased to 64.4 percent (from 67.0 percent). Rates of both public and private coverage remained stable in non-expansion states at 25.2 percent and 59.6 percent, respectively.
Impact of COVID-19 on NHIS 2020 and 2021 data
Though NCHS notes that data collection efforts for the 2020 NHIS were disrupted by the COVID-19 pandemic and, subsequently, estimates for April-December 2020 may have been impacted by nonresponse bias, normal survey collection and follow-up operations resumed in full by September 2020. All subsequent estimates presented in this early release report for January-June 2021 meet NCHS standards of reliability as specified in “National Center for Health Statistics data presentation standards for proportions.”1
Notes
All differences described in this analysis are statistically significant at the 95% confidence level, unless otherwise indicated.
Estimates are representative of the civilian noninstitutionalized U.S. population, and comparisons presented here are between NHIS data for January-June 2021 and January-June 2020.
1 Cohen, R.A., Martinez, M.E., Cha, A.E., & Terlizzi, E.P. (November 2021). Health insurance coverage: Early release of estimates from the National Health Interview Survey, January–June 2021. National Center for Health Statistics (NCHS). https://www.cdc.gov/nchs/data/nhis/earlyrelease/insur202111.pdf
Blog & News

2021 NHIS Early Release: Stable uninsured rate paired with increase in public coverage and decrease in private coverage
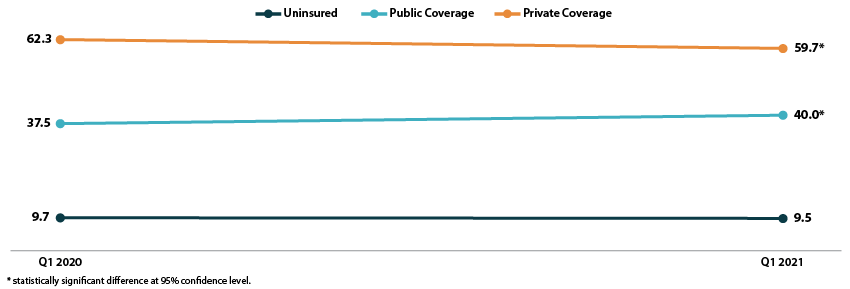
October 14, 2021:The National Center for Health Statistics (NCHS) has released quarterly estimates of health insurance coverage from January 2020-March 2021 from the National Health Interview Survey (NHIS) as part of the NHIS Early Release Program. These are some of the first estimates of health insurance coverage during 2021 from a major, federal government survey. This post compares uninsurance, private coverage, and public coverage rates in the first quarter of 2021 (Q1 2021) to those rates in the first quarter of 2020 (Q1 2020) and focuses on coverage by age group and federal poverty level (FPL).
Uninsured rates were stable among all age groups; Public and private coverage saw significant changes among all age groups
The uninsured rate remained stable in the first quarter of 2021, at an overall 9.5 percent for all ages, 11.3 percent for the non-elderly (age 0-64), 4.6 percent for children (age 0-17), and 13.8 percent for non-elderly adults (age 18-64).
All age groups except non-elderly adults saw increases in rates of public coverage. Public coverage increased 2.5 percentage points (PP) among all ages and for the non-elderly, increasing to 40.0 percent and 28.3 percent, respectively. Children saw an increase of 4.7 PP, rising to 45.6 percent with public coverage in Q1 2021.
Rates of private coverage fell 2.6 PP to 59.7 percent in Q1 2021 for those of all ages. Rates of private coverage were statistically unchanged for other specified age groups.
Figure 1. Health insurance coverage by type (all ages), Q1 2020 vs. Q1 2021
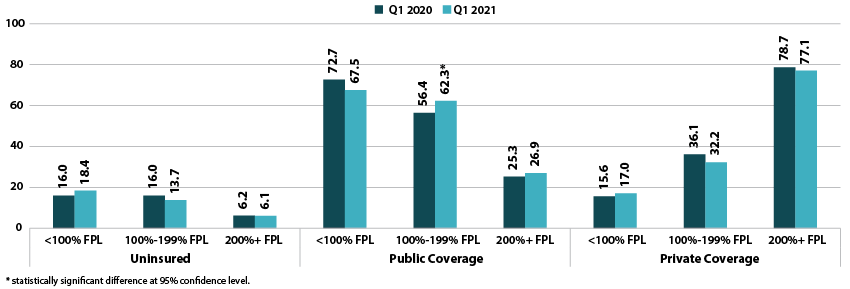
Coverage largely unchanged by poverty level
Rates of uninsurance were stable by poverty level in the first quarter of 2021. For those with incomes below 100% FPL, 18.4 percent were uninsured in Q1 2021. In other categories, 13.7 percent of those with incomes at 100%-199% FPL were uninsured, and 6.1 percent of those with incomes at or above 200% FPL were uninsured.
Rates of public coverage were statistically unchanged for those with incomes below 100% FPL (67.5 percent) and for those with incomes at or above 200% FPL (26.9 percent). Those with incomes 100%-199% FPL saw a 5.9 PP increase in rates of public coverage, rising to 62.3 percent in Q1 2021.
Rates of private coverage were stable by poverty level. Those with incomes below 100% FPL had a private coverage rate of 17.0 percent, those with incomes 100%-199% FPL had a private coverage rate of 32.2 percent, and those with incomes at or above 200% FPL had a private coverage rate of 77.1 percent.
Figure 2. Health insurance coverage by type by poverty level (all ages), Q1 2020 vs. Q1 2021
A note on changes to the NHIS data collection methodology
In response to the COVID-19 pandemic, the NHIS changed to a telephone-only and then telephone-first with in-person follow up data collection methodologies beginning on March 19, 2020. Though this did not affect the Q1 2020 estimates, NCHS’s analysis indicates that the change to telephone-only data collection led to an “over-representation of affluent households,” which may have affected the Q1 2021 estimates. More information on changes to federal survey methodology due to the COVID-19 pandemic is available in the SHADAC brief, Changes in Federal Surveys Due to and During COVID-19.
Publication
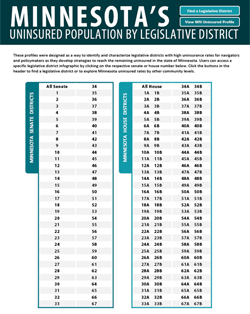
Minnesota's Uninsured Population by Legislative District
Our research team at SHADAC has continued its partnership with the Blue Cross Blue Shield Foundation of Minnesota to refresh a tool that provides critical information on the uninsured populations in Minnesota at the legislative district level.
Legislative District Infographics (2015-2019 data)
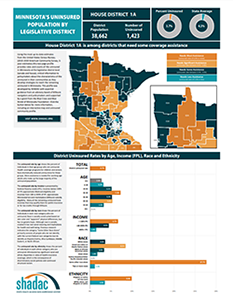
Using the United States Census Bureau's 2015-2019 American Community Survey, 5-year estimates, this unique set of infographics highlight and categorize uninsured rates using color-coded state maps and graphics that provide a deeper look into the socioeconomic data (such as race, ethnicity, income, and age) of each Minnesota House and Senate district. The state legislative maps are color-coded according to four levels of need for coverage assistance: Needs Most Assistance (uninsured rate of 6.9% or more); Needs Significant Assistance (uninsured rates between 4.6%-6.8%); Needs Some Assistance (uninsured rates between 2.4%-4.5%); Needs Less Assistance (under 2.3%). These infographics are designed to provide clear and concise snapshots of coverage needs to raise awareness and assist policymakers and health insurance navigators in developing strategies to reach the remaining uninsured in the state of Minnesota.
Click on an individual house or senate district in the PDF to the right to access a two-page infographic that contains detailed socioeconomic data about that respective district. If you need help determining a legislative district of interest, click the "Find a Legislative District" in the header of the accompanying PDF.
Interactive Map (2015-2019 data)
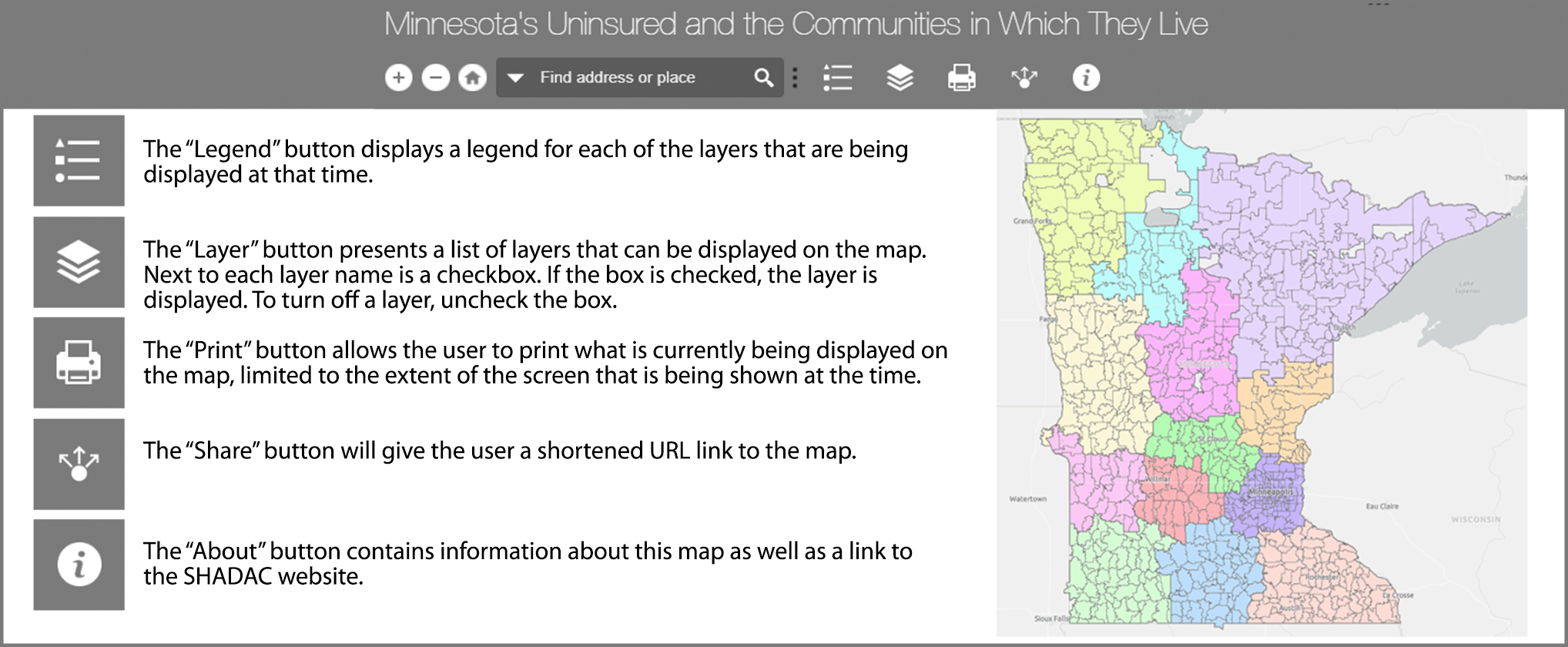 This map is designed to be used alongside the profile and contains data from the 5-year estimates within the United States Census Bureau's 2015-2019 American Community Survey. Use the “Find address or place” search box at the bottom of the map and then click on the magnifying glass.
This map is designed to be used alongside the profile and contains data from the 5-year estimates within the United States Census Bureau's 2015-2019 American Community Survey. Use the “Find address or place” search box at the bottom of the map and then click on the magnifying glass.
Click the image to the right to explore the interactive map.
We would greatly appreciate your feedback on the community and uninsured profile. Share your suggestions with us here.
Blog & News

Update to SHADAC’s Minnesota Uninsured Legislative District Infographics Aims to Assist in Addressing Coverage Disparities
September 23, 2021:Our research team at SHADAC has continued its partnership with the Blue Cross Blue Shield Foundation of Minnesota to refresh a tool that provides critical information on the uninsured populations in Minnesota at the legislative district level. Using the most up-to-date estimates available from the United States Census Bureau, (2015-2019 American Community Survey, 5-year estimates) this unique set of infographics are designed to identify and categorize legislative districts with high uninsured rates using color-coded state maps and graphics that provide a deeper look into the socioeconomic data of each Minnesota House and Senate district.
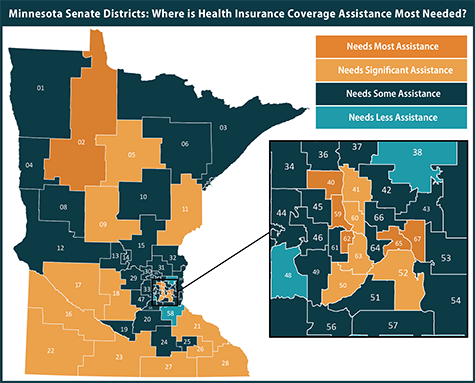 In these updated infographics, state legislative maps are color-coded according to four levels of need for coverage assistance: Needs Most Assistance (uninsured rate of 6.9% or more); Needs Significant Assistance (uninsured rates between 4.6%-6.8%); Needs Some Assistance (uninsured rates between 2.4%-4.5%); Needs Less Assistance (under 2.3%).
In these updated infographics, state legislative maps are color-coded according to four levels of need for coverage assistance: Needs Most Assistance (uninsured rate of 6.9% or more); Needs Significant Assistance (uninsured rates between 4.6%-6.8%); Needs Some Assistance (uninsured rates between 2.4%-4.5%); Needs Less Assistance (under 2.3%).
Users are able to click on an individual district in the accompanying PDF to access a two-page infographic that contains detailed socioeconomic data about that respective district's uninsured population, such as race, ethnicity, income, and age. These infographics are designed to provide clear and concise snapshots of coverage needs to raise awareness and assist policymakers and health insurance navigators in developing strategies to reach the remaining uninsured in the state of Minnesota.
“While uninsured data for Minnesota are available elsewhere, the data we’ve compiled within these customized infographics are the most explicit in calling out levels of need and addressing disparities within the state,” Dr. Kathleen Call explains. “We felt that it was most important to highlight these categories of need at the legislative district level because that is where policy is made and where our data would be most useful.”
For additional information on the original uninsured profile tool, users can access the Resource Page on our SHADAC website where the tool is available for download in Excel spreadsheet format. In addition to these infographics, the profile tool is accompanied by an interactive map that shows users the geographic makeup of each specified region in relation to schools, hospitals, native reservations, and other important or distinctive landmarks. Users are also able to use the site to provide feedback on the current profile tool, and can also request that a similar tool be built specifically for their state.

