 VISIT STATE HEALTH COMPARE
VISIT STATE HEALTH COMPARE
Blog & News





SHADAC Responds to Proposed American Community Survey (ACS) Sexual Orientation and Gender Identity (SOGI) Test Questions
December 4, 2023:|
View the U.S. Census Bureau's full request for comments in the September 19th edition of the Federal Register. |
On September 19, 2023, the U.S. Census Bureau released a request for comments regarding the proposed addition of test questions regarding sexual orientation and gender identity (SOGI) for the American Community Survey (ACS). According to the notice in the Federal Register, the Census Bureau specifically hopes to test question wording, response categories, and placement within the survey itself.
Researchers at SHADAC reviewed the proposed test questions included in the Register proposal, as well as the methodology and reasoning behind the Census Bureau’s choices, and responded with comments regarding the measurement of sex and gender identity. Specifically, researchers discuss the limitations of the two-step gender identity questions, language and inclusivity concerns, and recommendations for a more streamlined and accessible two-step question format.
SHADAC’s Comments on Measuring Sex and Gender Identity
When designing survey questions, the consumer experience is paramount. Maximizing the accessibility and acceptability of question language improves data quality in multiple dimensions, including item non-response, misclassifications, and overall response rates.
In the case of measuring sex and gender identity, context matters. It is important to acknowledge how these questions might differ in various settings - when asked on a survey compared to when asked in an administrative or clinical setting, for example. We are concerned that the ACS is missing a key opportunity to update questions on sex and gender in ways that both enhance user experience and are specific to the survey setting.
The test questions for sex and gender identity as proposed use overly academic language that is better suited for a clinical setting, by asking first ‘what sex was NAME assigned at birth’ followed by ‘current gender identity.’ While such questions have utility, such as for verification of specific health insurance benefits, this approach is not optimal for a population survey such as the ACS.
Unnecessary jargon makes questions less accessible for respondents with lower literacy levels or who are non-English speaking and adds to the cognitive burden for all respondents. Survey language should minimize the respondent burden in order to support data quality and user experience. The limitations of the proposed two-step gender identity question have been described by the National Academies of Sciences, Engineering, and Medicine (NASEM).
Specific concerns worth highlighting are:
1) The proposed response options for ‘current gender’ are not inclusive of transgender experiences because these options imply that transgender is a tertiary or ‘other’ category and mutually exclusive from male or female identities. Allowing for multiple answers (one of the proposed test options) does not address this conceptual limitation.
2) Asking chronologically about ‘sex assigned at birth’ followed by ‘current gender identity’ may be perceived as invasive and/or invalidating for transgender respondents, which could increase item nonresponse for this critical population.
3) Asking a third question for verification of gender status when a respondent’s answers to ‘sex assigned at birth’ and ‘current gender’ don’t match places an undue burden on the transgender and nonbinary population. At minimum, the testing process should assess false positive rates and seek to avoid unnecessarily burdensome questioning of transgender and nonbinary people.
4) ‘Sex assigned at birth’ is not inclusive of intersex or nonbinary designations on infant birth certificates. These situations are increasingly common, and the current wording could lead to false positives for transgender, along with unnecessarily invasive questioning among individuals born with intersex traits.
SHADAC recommends that the Census consider a more streamlined two-step question approach that gathers the same information (sex assigned at birth and current gender) while providing a more inclusive and accessible experience for respondents. Specifically, we recommend asking first ‘what is your gender’ followed by ‘are you transgender.’ This approach was developed in Oregon via extensive stakeholder engagement. Similar language has also been used by administrators to update population survey questions in Minnesota.
The alternative two-step question addresses the limitations described above in the following ways:
1) Response options for ‘gender’ should include male, female, nonbinary, and a write-in response option. Asking about transgender identity in a separate question avoids portraying transgender as mutually exclusive with male or female. For respondents who need an explanation for ‘transgender,’ a hover box or an interviewer can provide a definition as follows: ‘Transgender describes a person whose gender identity differs from their sex assigned at birth.’
2) Asking simply about ‘gender’ first is clear and inclusive. Avoiding the ‘sex assigned at birth’ initial question would be less duplicative and more accessible for many respondents.
3) Asking directly about transgender identity (with ‘yes/no’ response options) prioritizes accessible language to minimize respondent burden and may eliminate the need for additional verification for transgender respondents. Ethically, the ACS should avoid asking all transgender respondents for extra verification without strong data to indicate that doing otherwise would lead to significantly elevated false positive rates.
4) Not asking about ‘sex assigned at birth’ avoids unnecessary collection of personal health data. This supports privacy for all respondents. Additionally, this approach could help reduce item nonresponse and false positives among intersex individuals as well as cisgender respondents who are unfamiliar with and/or dislike the language and concepts in the initially proposed test questions.
Thank you for your consideration. We know that the Census Bureau faces many important decisions and appreciate the chance to share our feedback on this important content test.
Publication
Disparities in Minnesota's COVID-19 Vaccination Rates
Health inequities are nothing new in the U.S., but the COVID pandemic has placed them in a new light. Numerous studies have reported disparities in how COVID-19 affects many vulnerable groups, often placing them at higher risk of infection, hospitalization, and death. And the inequitable effects of the disease itself are not the only cause for alarm. Once COVID-19 vaccines received authorization, equitable vaccination initiatives became a concern, especially as surveys indicated widespread hesitancy and lagging uptake.
Partnering with the Minnesota Electronic Health Record Consortium, SHADAC delved deep into an analysis of COVID-19 vaccination rates in Minnesota, examining not only point-in-time measures of vaccine disparities but also measuring how quickly the state reached vaccination thresholds for different subpopulations. This webinar will present findings from the study, including analysis of disparities in time-to-vaccination by race and ethnicity, age, and other demographic categories.
Attendees learned about:
- Disparities in COVID-19 vaccination rates across demographic groups
- How policymakers' vaccine prioritization approach may have contributed to health inequities
- Ideas for improved metrics for measuring time-sensitive interventions during public health emergencies
Speakers

Colin Planalp, Speaker
SHADAC
Colin Planalp, MPA, senior research fellow at SHADAC and author on the analysis, will present data published in a recent brief. He will be joined by Tyler Winkelman, MD, MSc, past-President of the consortium and co-director of the Health, Homelessness, and Criminal Justice Lab at Hennepin Healthcare Research Institute. Dr. Winkelman will discuss the Minnesota EHR Consortium and its unique data source, which made the study’s time-to-vaccine analysis possible.
|

Dr. Tyler Winkelman, Speaker
Hennepin Healthcare Research Institute
Dr. Tyler Winkelman is the Past-President of the Minnesota Electronic Health Record Consortium and co-director of the Health, Homelessness, and Criminal Justice Lab at Hennepin Healthcare Research Institute. Dr. Winkelman is also the General Internal Medicine Division Chief at Hennepin Healthcare. He leads the Consortium’s COVID-19 Project, a statewide collaboration with the Minnesota Department of Health to track COVID-19 prevalence, testing, and vaccination among racial and ethnic groups, as well as people experiencing homelessness and/or incarceration.
|
Related Resources
- Webinar slides from SHADAC
- Disparities in Minnesota's COVID-19 Vaccination Rates (Brief)
- Full Transcript
Blog & News

California Achieves Lowest Uninsured Rate Ever in 2022 (Cross-Post)
November 13, 2023:The following blog is cross-posted from The California Health Care Foundation.
Author: Lacey Hartman, Senior Research Fellow, SHADAC
Maintaining Gains Hinges on Transitioning People Who Lose Medi-Cal to Other Coverage in Coming Months
The share of Californians under age 65 (“nonelderly”) without health insurance reached a historic low in 2022. Based on the most recent California Health Interview Survey (CHIS), the percentage of nonelderly Californians without health insurance dropped to 6.2% in 2022, a statistically significant decline from 2021 (7.4%). The rate of nonelderly people without coverage for a year or more also reached a historic low in 2022. Commonly called the “long-term uninsured,” their rate dropped from 5.7% in 2021 to 4.5% in 2022, another statistically significant decline.

Disparities in Coverage by Race and Ethnicity Narrow, but Inequities Persist
California’s Latino/x population experienced the largest improvement in coverage between 2021 and 2022; the share who reported being uninsured at the time of the survey dropped from 11.4% in 2021 to 9.1% in 2022, a change that was statistically significant. The Latino/x rate in 2022 also represents a historic low for this group.
The uninsured rate for White Californians also declined by a statistically significant but smaller amount, from 3.6% to 2.8%. There were no other statistically significant changes between 2021 and 2022 by race/ethnicity. Although there have been important gains in narrowing disparities in coverage by race and ethnicity in the state, Latino/x Californians continue to be uninsured at rates triple that of their White counterparts. Black and Asian Californians are uninsured at twice the rate of White Californians. Due to small sample sizes for American Indians and Native Hawaiian / Pacific Islanders in the survey, it was not possible to produce reliable uninsured rates for those groups.

Discussion
The fact that fewer nonelderly Californians were without coverage in 2022 than ever before is clearly good news. However, in 2023, the federal continuous coverage requirement for Medicaid came to an end. It’s estimated that as many as 2–3 million Californians may leave Medi-Cal as a result. How many Californians ultimately lose their Medi-Cal coverage and whether those leaving the program get connected to other coverage will have a huge impact on the state’s uninsured rate going forward.
These issues — as well as other challenges, such as inflation — may make holding onto California’s coverage gains difficult in the coming years. It will be vital to continue monitoring data from 2023 and future years to fully understand the impact of the pandemic — and the end of associated coverage protections, as well as other policy changes — on California’s health coverage landscape.
Blog & News

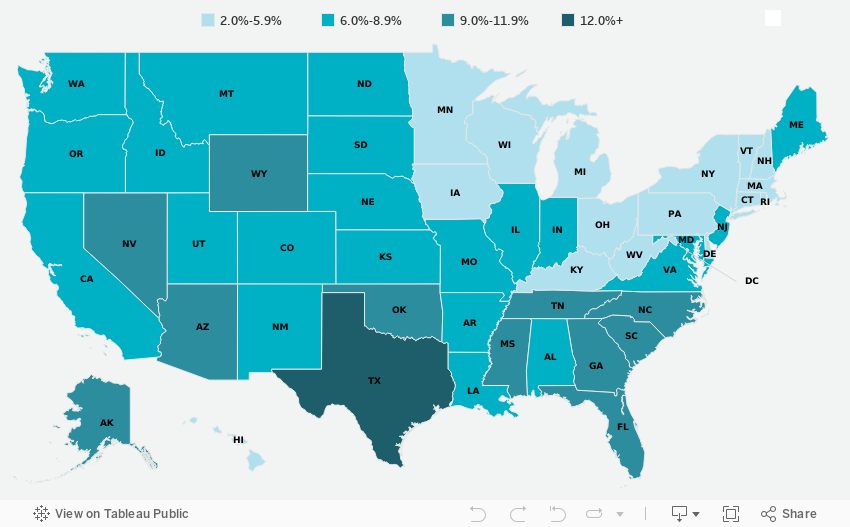
2022 ACS Tables: State and County Uninsured Rates, with Comparison Year 2021
November 17, 2023:Each year, SHADAC uses data released from the American Community Survey (ACS) via the U.S. Census Bureau's data.census.gov tool to produce estimates of uninsurance at the state and county level.*
Click on a state below in the interactive map to see a PDF table of uninsured rates by state and sub-state geographies, but also by demographic characteristics (e.g., age, race/ethnicity, and poverty level) for 2022 and comparison year 2021.
Click here to view uninsurance estimates for the United States.
Click here to view uninsurance estimates for Puerto Rico and its municipios.
Note: These tables present uninsured rates, which indicate the share of the population that is uninsured. For example, a 10 percent uninsured rate for adult women indicates that 10 percent of all adult women are uninsured.
Maps & Tables of Private, Public, & Uninsured Changes from 2021 to 2022
- Private Coverage Rates by State, Change from 2021 to 2022, for All People
- Public Coverage Rates by State, Change from 2021 to 2022, for All People
- Uninsurance Rates by State, Change from 2021 to 2022, for All People
About the ACS
The ACS is a household survey that began in 2005 and produces annually updated data on a variety of population characteristics, including health insurance coverage. In total, the ACS surveys approximately three million U.S. households each year. An important feature of the ACS is that it includes a large enough sample for state‐level and sub‐state estimates.
The ACS began asking survey respondents about health insurance coverage during the 2008 calendar year. Specifically, the survey asks respondents about current coverage for each person in the respondent’s household. A person is categorized as “insured” if he or she has coverage at the point in time at which the survey is administered.
*Why Aren’t Estimates Provided for All Counties?
Due to sample size constraints, single-year ACS estimates are available at the county level only for counties with a population greater than 65,000.
How Are These Estimates Different from the Estimates that SHADAC Publishes Using Census Bureau Micro-Data Files?
Two definitions used by the Census Bureau to generate the tabulations above differ from those that SHADAC uses to generate tabulations for State Health Compare. The definitional differences are as follows:
Family
The Census Bureau defines a family as “all related people in a household.”
SHADAC defines a family using a measure called the “Health Insurance Unit” (HIU), which includes all individuals who would likely be considered a family unit in determining eligibility for either private or public coverage.
To learn more about the 2020 update of SHADAC's Health Insurance Unit (HIU) see our HIU resource page, which houses two issue briefs: The first describes the SHADAC HIU, its purpose, the most recent update, and improvements to HIU data inputs; and the second outlines the impacts of using the SHADAC HIU in analysis so that researchers can assess whether the SHADAC HIU is suitable for their research and what the potential impacts of its use might be. The page also provides a link to STATA and SAS codes to aid in the use of the HIU variable.
Family Income
The Census Bureau determines family income as a percentage of the Federal Poverty Level (FPL), which is a definition of poverty used primarily for statistical purposes. For example, FPL is used to estimate the number of Americans living in poverty each year.
SHADAC determines family income as a percentage of the U.S. Department of Health and Human Services’ Federal Poverty Guidelines (FPG), which is a measure used for administrative purposes. For example, FPG is used to determine eligibility for federal programs such as Medicaid and the Supplemental Nutrition Assistance Program (SNAP).
To learn more about the difference between FPL and FPG, read our updated blog post from April 2023.
Related ACS Materials:
- An Annual Conversation with the U.S. Census Bureau: 2022 Health Insurance Coverage Estimates from the ACS and CPS
- 2022 ACS: Declining Uninsured Rates for the U.S. and States are Supported by Private and Public Coverage Increases
- CPS ASEC: 2022 National Health Insurance Coverage Estimates Show Falling Rates of Uninsurance and Direct-Purchase Coverage (Infographic)
Publication
Federal Survey Sample Size Analysis: Disability, Language, and Sexual Orientation and Gender Identity
 The Medicaid and CHIP Payment and Access Commission contracted with the State Health Access Data Assistance Center (SHADAC) to conduct a review and sample size analysis of 13 federal population health surveys to assess the quality and availability of data for certain populations facing health inequities, including people with disabilities, language access needs, and people who indicate their sexual orientation or gender identity (SOGI). This brief provides an overview of each federal survey and identifies which surveys included questions about disability, primary language, limited English proficiency (LEP), and sexual orientation and gender identity (SOGI). Below is an overview table of the Federal surveys included in this analysis.
The Medicaid and CHIP Payment and Access Commission contracted with the State Health Access Data Assistance Center (SHADAC) to conduct a review and sample size analysis of 13 federal population health surveys to assess the quality and availability of data for certain populations facing health inequities, including people with disabilities, language access needs, and people who indicate their sexual orientation or gender identity (SOGI). This brief provides an overview of each federal survey and identifies which surveys included questions about disability, primary language, limited English proficiency (LEP), and sexual orientation and gender identity (SOGI). Below is an overview table of the Federal surveys included in this analysis.
| Federal Survey | Periodicity | Target Population | States, DC, and Territories Represented | Most Recent Data Year | Total Population Unweighted Sample Size | Total Unweighted Sample Size for Medicaid 1 |
|---|---|---|---|---|---|---|
| ACS | Annual | Civilian, non-institutionalized U.S. population | 50 states, D.C., Puerto Rico | 2021 | 3,252,599 | 434,900 |
| BRFSS | Annual | U.S. adults > 18 years | 49 states (no Florida in 2021), D.C., Guam, Puerto Rico, Virgin Islands | 2021 | 438,693 | 50,306 |
| CPS | Annual | Civilian, non-institutionalized U.S. population | 50 states, D.C. | 2022 | 152,732 | 24,155 |
| HPS | Panel | U.S. adults > 18 years | 50 states, D.C. | 2023 | 59,290 | 2,764 |
| MEPS-HC2 | Panel | Civilian, non-institutionalized U.S. population | No state estimates | 2020 | 27,805 | 6,504 |
| MCBS3 | Annual | All individuals enrolled in Medicare | No state estimates | 2020 | 13,916 | 2,593 |
| NAMCAHPS4 | Fielded once | Adults enrolled in Medicaid | 50 states, D.C. | 2014 | 272,679 | 272,679 |
| NHANES | Periodic | Civilian, non-institutionalized U.S. population | No state estimates | 20205 | 9,254 | 2,841 |
| NHIS | Annual | Civilian, non-institutionalized U.S. population | 50 states, D.C. when two years combined in the RDC | 2022 | 35,115 | 4,918 |
| NSCH6 | Annual | U.S. children < 18 years | 50 states, D.C. when two years combined | 2021 | 50,892 | 11,259 |
| NSDUH | Annual | Civilian, non-institutionalized U.S. population, age 12 + | No state estimates | 2021 | 58,034 | 11,008 |
| PRAMS | Annual | Pregnant women in 47 states, D.C., and Puerto Rico | See target population | 2021 | NA | NA |
| SIPP7 | Panel | Civilian, non-institutionalized U.S. population | 50 states, D.C. | 2022 | 40,510 | 5,835 |
1 Unless otherwise noted, where relevant, Medicaid was defined using the typical MACPAC hierarchy:
(1) Medicare; (2) Private with no Medicare; (3) Medicaid with no Medicare or private; (4) Other type of insurance with no Medicare or private; (5) Uninsured all year
2 Medicaid coverage was defined based on the most recent date of data collection (e.g., December).
3 MCBS data uses “full year dual” to define Medicaid, meaning people who were enrolled in Medicare and Medicaid all year.
4 NAMCAHPS limited to adults enrolled in Medicaid.
5 Sample size analysis conducted using 2017-2018 file, because of pandemic impacts on data collection in 2020.
6 The NSCH includes three categories of children’s coverage (public, private, uninsured); we code children in public coverage as having Medicaid, because Medicare is much less common among children.
7 SIPP data uses the annual coverage variables to define Medicaid.
Source: SHADAC analysis of federal survey data.
The findings show that the majority of surveys include questions to identify individuals with a functional disability. Still, fewer than half of these surveys include questions about intellectual disability, serious mental illness, primary language, LEP, and SOGI. Of the surveys that include these questions, the majority have a sufficient sample for reporting about Medicaid-covered individuals for each demographic group.

