 VISIT STATE HEALTH COMPARE
VISIT STATE HEALTH COMPARE
Publication



State Medicaid Member Experience Qualitative Data Scan
As part of the ongoing work in Phase 2 of the Medicaid Equity Monitoring Tool project, SHADAC researchers have been working to understand what available data sources and measures currently exist that could be useful in populating a potential Medicaid Equity Monitoring Tool.

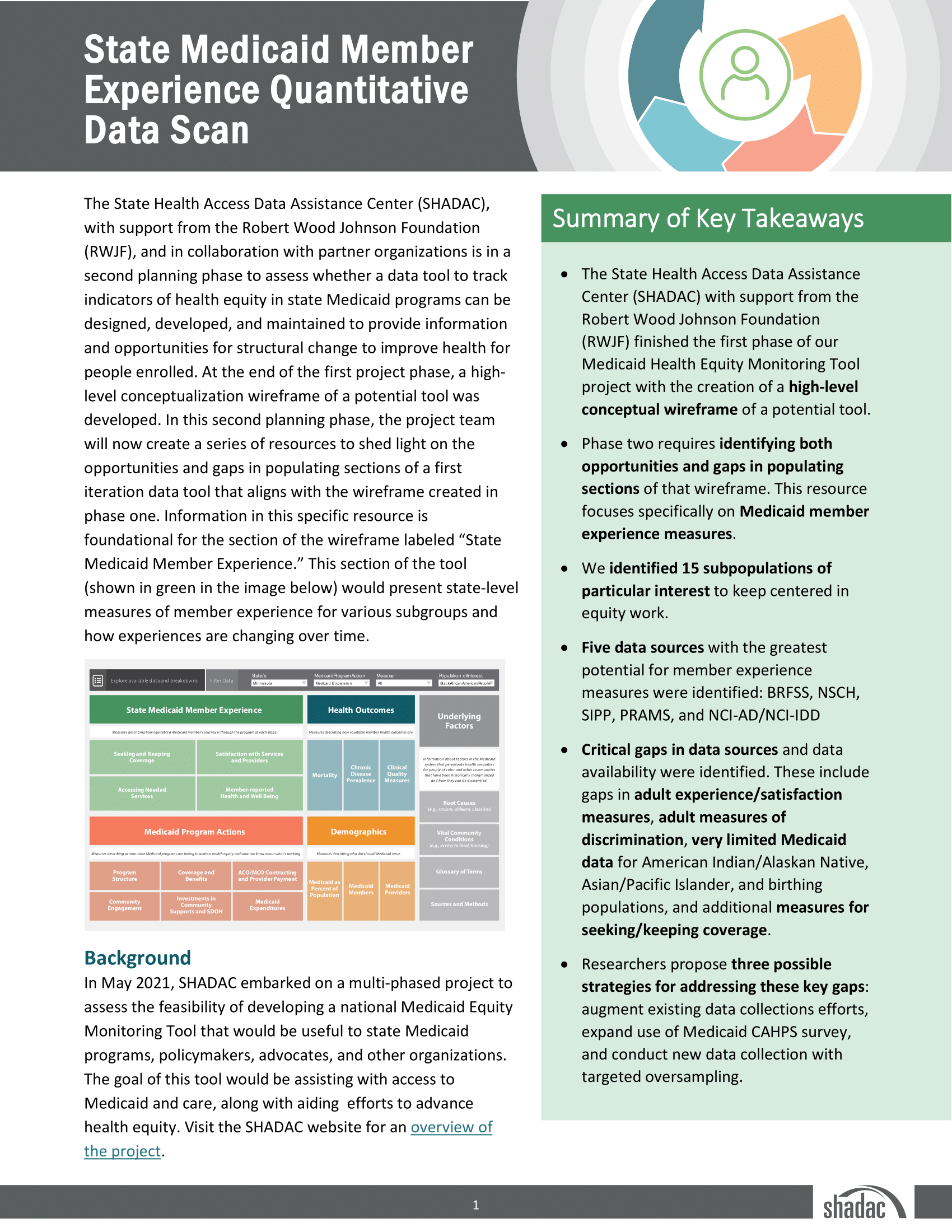
In Phase 1, the project team conceptualized a high-level wireframe, displaying what such a tool could look like, and how measures could be included and categorized. Currently, five general categories have been proposed - State Medicaid Member Experience, Health Outcomes, Medicaid Program Actions, Demographics, and Underlying Factors - further stratified into various domains, under which individual measures could be housed.
In the case of State Medicaid Member Experience, the category of focus for SHADAC’s initial data scan, four domains have been proposed:
- Accessing Needed Services
- Member-Reported Health and Well Being
- Satisfaction with Services and Providers
- Seeking and Keeping Coverage
In starting the initial data scan process, SHADAC has already faced a number of critical decision points – first and foremost, where to begin.
With five main categories and a multiplicity of potential domains under each, there were numerous points of entry into a process we hoped would help to gain a better understanding of the potential measures currently available (as well as a process to identity gaps in such data collection) to populate a tool.
After deciding to start with the Medicaid Member Experience category, a secondary decision split the data scan process into two parts, quantitative and qualitative.1 A resource documenting the quantitative data scan's process, findings, and further recommendations was published in January 2024. This new resource examines the qualitative aspects of Member Experience through identification of related research studies.
Top-level findings reveal that there are few sources documenting qualitative data collection methods regarding the experiences of Medicaid enrollees – our scan found just 21 – even fewer that focus specifically on our project’s 15 identified subpopulations of interest, and even fewer studies conducted over extended periods of time (2).
In addition to a summation of the scan results, the resource also contains an appendix table that crosswalks each source to all relevant measurement domains (e.g., Accessing Needed Services, Member-reported Health and Well Being, Satisfaction with Services and Providers, Seeking and Keeping Coverage, and Discrimination), provides relevant quotes from either Medicaid members themselves or their representatives, and includes population demographics such as race/ethnicity, disability status, and geographic location, among others.
Click on the image above to access the full report, or access it at this link.
[1] For more on the decision-making process regarding the initial data scan, please see the State Medicaid Member Experience Quantitative Data Scan page.

Blog & News

New Data on Health Insurance Coverage by Race/Ethnicity Added to State Health Compare
June 28, 2024:State Health Access Data Assistance Center (SHADAC) has added two new racial/ethnic population groups to our measures of health insurance coverage available on State Health Compare.
Using micro-data from the American Community Survey (ACS), we were able to add health insurance coverage measures for American Indian/Alaska Native (AIAN) and Native Hawaiian Pacific Islander (NHPI) populations. Specifically, SHADAC has added insurance coverage data for AIAN and NHPI populations at both the national and state level (when sample size permits) from the years 2008-2022. Estimates for these groups are also available by age and poverty status.
This update now allows users to download estimates of insurance coverage for all of the minimum race categories for data collection outlined by the Office of Management and Budget (OMB), which are: American Indian or Alaska Native (AIAN), Asian, Black or African American, Native Hawaiian or Other Pacific Islander (NHPI), and White.
| Uninsured adults (19-64) in the US, 2021-2022 | ||||||
|---|---|---|---|---|---|---|
| Race/ethnicity | Age | 2021 | 2022 | Difference | * | |
| AIAN | 19-64 | 24.5% | 22.2% | -2.4 | * | |
| African-American / Black | 19-64 | 13.4% | 12.1% | -1.3 | * | |
| Asian | 19-64 | 7.2% | 6.7% | -0.5 | * | |
| Hispanic / Latino | 19-64 | 24.4% | 22.8% | -1.5 | * | |
| NHPI | 19-64 | 12.1% | 13.6% | 1.5 | ||
| Other / Multiple Races | 19-64 | 11.2% | 10.5% | -0.7 | * | |
| White | 19-64 | 8.2% | 7.4% | -0.7 | * | |
| All | 19-64 | 12.0% | 11.2% | -0.9 | * | |
| * Significant difference between years. Source: SHADAC analysis of the 2021-2022 American Community Survey. |
||||||
In this analysis, we used this newly available data from State Health Compare to examine differences in uninsurance from 2021 to 2022 by race/ethnicity for adults ages 19-64. Over this period, the overall uninsured rate for non-elderly adults dropped nearly a percentage point, reaching 11.2%. The largest drop in uninsurance was seen among AIAN adults, lowering by 2.4 percentage points. Hispanic and Black adults also saw improvements in coverage of greater than one percentage point (1.5 and 1.3 percentage points, respectively). More modest gains in coverage were reported by adults who were White, Asian, and Other/Multiple races.
Significant decreases were seen consistently across populations by race/ethnicity except for the NHPI adult population, which did not see this same decrease in uninsurance. While estimates were limited by sample size and changes were not significant, uninsurance rates for this group increased from 12.1% to 13.6%. These concerning rates of uninsured NHPI adults contrasted with the overall trend of decreased uninsurance rates and thus warrant further observation.
While encouraging to see a trend of decreasing uninsurance amongst non-elderly adults, disparities in insurance coverage between racial/ethnic groups are persistent. For example, in 2022, more than one in five adults were uninsured among both the Hispanic/Latino and AIAN populations. Uninsurance was also high for NHPI and Black adults, at 13.6% and 12.1%, respectively. The substantial differences in coverage between racial/ethnic populations illustrate the ongoing priority of improving health equity, including health care access. We plan to continue monitoring insurance coverage in light of ongoing post-pandemic policy changes. Providing more granular estimates by race/ethnicity will support efforts to understand and reduce disparities in health care access.
Blog & News

Revised Childhood Vaccinations Measure on State Health Compare Shows Vaccination Rates Vary by State, Race/Ethnicity, and Insurance Coverage
January 30, 2024:Introduction
Childhood Vaccinations are an effective way to protect infants and young children from harmful diseases that can cause serious illness or death. Children are commonly vaccinated against a number of diseases, including chickenpox (Varicella), polio, hepatitis A and B, and measles, mumps, and rubella (MMR).
Despite the well-documented safety and efficacy of the vaccines, along with the endorsement of child vaccinations by the Centers for Disease Control and Prevention (CDC) and other public health authorities, rates of child vaccination lag in some portions of the United States. Monitoring trends in child vaccination rates can help explain why such gaps exist and inform efforts to improve child vaccination rates in the U.S.
A revised child vaccination measure on SHADAC’s State Health Compare (SHC) now presents annual, state-level vaccination rates for children aged 35 months, specifically the percent of those children who received the full series of recommended vaccines using data from the National Immunization Survey (NIS-Child) by survey year. This measure also presents these state-level rates by race and ethnicity, health insurance coverage type, and poverty level. In this blog post, SHADAC researchers highlight key findings from this new child vaccinations measure by race and ethnicity and type of health insurance coverage.
The Share of Children Receiving Recommended Vaccinations Has Been Relatively Stable, Though Large Variation Exists Across States
Nationally between 2017 and 2021, the share of children aged 35 months who had received the full schedule of recommended vaccinations remained relatively stable, remaining between 70% and 73% nationwide.
National Child Vaccination Rates, 2017–2021
However, while stable nationally, there was substantial state variation in the share of children who had received recommended vaccinations. For example, in 2021, the national child vaccination rate sat at 72.1%, but state-level rates ranged from as low as 56.6% in West Virginia to as high as 87.9% in Iowa. Also in 2021, six states (CT, IA, MD, MA, ND, and VT) had child vaccination rates of 80% or greater while West Virginia was the only state with a vaccination rate below 60%.
Top Five and Bottom Five State Child Vaccination Rates, 2021
| Top Five States | Iowa | 87.9% |
|---|---|---|
| Massachusetts | 85.4% | |
| Connecticut | 84.0% | |
| Vermont | 82.1% | |
| North Dakota | 81.3% | |
| United States | 72.1% | |
| Bottom Five States | West Virginia | 56.6% |
| Alaska | 61.3% | |
| Louisiana | 62.0% | |
| Arizona | 62.2% | |
| Georgia | 63.3% | |
Black Children, Hispanic/Latino Children, and Children of Other or Multiple Races Were Less Likely to Have Received Recommended Vaccinations Compared to White Children
Nationally, there were significant gaps in the share of children who had received the recommended vaccines by age 35 months by race and ethnicity.1
Non-Hispanic White children had the highest rate of vaccination at 75.5%, followed by children of multiple races or some other race (non-Hispanic) at 72.8%, Hispanic/Latino children (any race) at 69.9%, and, finally, African-American/Black children at 66.5%.
National Child Vaccination Rates by Race and Ethnicity, 2019–2021
There were also large gaps in rates of child vaccinations by race and ethnicity at the state level in 2019–2021, as shown in the table below. For example, in Michigan, African-American/Black children were nearly 30 percentage points less likely to have received the full schedule of recommended vaccinations compared to White children (49.8% vs. 79.3%). In the District of Columbia, Hispanic/Latino children were more than 20 percentage points less likely to have received the recommended vaccinations compared to White children (62.1% vs. 82.5%). And in North Dakota, children of some other race or multiple races were 20 percentage points less likely to have received the recommended vaccinations compared to White children (60.1% vs. 80.1%).
States with statistically significant gaps in child vaccination rates by race and ethnicity, 2019–2021
| State | White | African-American / Black | Hispanic / Latino | Other / Multiple Races |
|---|---|---|---|---|
| United States | 75.5% | 66.5%* | 69.9%* | 72.8%* |
| Dist. of Columbia | 82.5% | 68.1%* | 62.1%* | 70.8% |
| Georgia | 75.2% | 57.8%* | 69.8% | 70.8% |
| Illinois | 79.3% | 61.3%* | 66.9%* | 75.9% |
| Indiana | 73.1% | 66.0% | 59.1%* | 70.4% |
| Louisiana | 70.1% | 58.5%* | 69.3% | 71.9% |
| Maryland | 84.5% | 75.7%* | 71.4%* | 77.7% |
| Michigan | 79.3% | 49.8%* | 76.7% | 72.8% |
| Nevada | 76.4% | 55.8%* | 73.2% | 72.7% |
| New Jersey | 76.1% | N/A | 59.6%* | 72.2% |
| New Mexico | 76.6% | N/A | 67.7%* | 72.6% |
| New York | 69.8% | 69.0% | 67.0% | 79.5%* |
| North Dakota | 80.1% | N/A | N/A | 60.1%* |
| Oklahoma | 75.2% | N/A | 71.1% | 59.5%* |
| Rhode Island | 81.7% | N/A | 70.6%* | 83.1% |
| Tennessee | 75.9% | 49.4%* | 59.9%* | 76.6% |
| Texas | 71.0% | 61.7%* | 72.2% | 70.1% |
|
* Statistically significant difference (95% confidence level) in state estimate compared to Whites Source: SHADAC analysis of 2019–2021 NIS-Child microdata N/A indicates that data were not available or were suppressed due to statistical unreliability or small sample size |
||||
Health Insurance Coverage Matters for Rates of Child Vaccinations
Nationally, during the years 2020 through 2021, there were substantial gaps in the share of children who had received the recommended vaccinations by source of health insurance coverage. Children with private coverage alone (e.g., employer-sponsored or direct-purchase coverage) had the highest rate of vaccination coverage at 80.3%. Children with some other insurance (Children's Health Insurance Plan [CHIP] coverage, Indian Health Service [IHS] coverage, military, or some other form of insurance alone or in combination with private insurance) had a vaccination rate of 70.7%. Children with any Medicaid coverage (alone or in combination with other coverage) had a vaccination rate of 66.2%, 14 percentage points lower than private coverage. Children with no health insurance coverage (i.e., uninsured) had by far the lowest vaccination rate at 50.0%, which is more than 30 percentage points lower than children with private coverage alone.
National Child Vaccination Rates by Coverage Type, 2020–2021
That national pattern holds across the states, though due to small sample sizes, there are few available state-level estimates for children with other insurance and uninsured children. The chart below compares rates of vaccinations for children with private coverage alone and children with any Medicaid coverage. Rates of vaccinations among children with Medicaid were lowest in Alaska at 53.1% and highest in Connecticut at 81.1%. Child vaccination rates among children with Medicaid were at or below 60%in five states—AK, CO, KS, LA, and NJ—and were at or above 80% in just two states—Connecticut and Iowa. Rates of vaccinations among children with private coverage alone ranged from the lowest at 74.2% in Minnesota to the highest at 90.3% in Iowa.
In 35 states, children with any Medicaid coverage were less likely to have received recommended vaccinations compared to children with private coverage alone. Colorado had the largest percentage point gap between children with private coverage alone and any Medicaid coverage at 23.4 (82.4% vs. 59.0%), while Nebraska had the smallest gap at 1.5 percentage points (not statistically significant, 79.8% vs. 78.3%).
Data and Methods
Estimates of child vaccination rates represent the share of children aged 35 months who have received all recommended vaccinations, including the full series of DtaP, poliovirus, measles-containing, Hib, HepB, varicella, and PCV vaccines, which together provide protection against diphtheria, pertussis, tetanus, poliovirus, measles, mumps, rubella, hepatitis b, haemophilus influenza b, chicken pox, and pneumococcal infections.
Data in this post come from SHADAC’s revised Child Vaccinations measure on State Health Compare, which are based on our analysis of National Immunization Survey-Child (NIS-Child) microdata produced by the Centers for Disease Control and Prevention.
Three years of data were pooled to produce estimates by race and ethnicity; two years of data were pooled to produce estimates by coverage type. In both cases, this was done to increase sample sizes at the state level for smaller populations and to increase the number of statistically reliable state estimates. Estimates represent an average for these periods.
Note that the data source used in this analysis (NIS-Child) does not make data by more detailed race and ethnicity categories available. It is likely that these available categories conceal important differences within the aggregate groups, particularly the “some other race / multiple races” category. This group is likely to be primarily composed of children of different racial and ethnic groups in different states. Further, estimates were not available for all states for all racial and ethnic groups due to small sample sizes, even when pooling multiple data years.
Unless otherwise specified, all differences described in this analysis are statistically significant at the 95% level of significance.
1 Race lacks a genetic basis—it is socially constructed based on skin color and “apparent” physical differences. While race is socially created, it does have real social meaning and implications for health and well-being, including access to important health care services, such as vaccinations.
Publication
State Medicaid Member Experience Quantitative Data Scan
As part of the ongoing work in Phase 2 of the Medicaid Equity Monitoring Tool project, SHADAC researchers have been working to understand what available data measures currently exist that could be useful in populating a potential Medicaid Equity Monitoring Tool.
In Phase 1, the project team conceptualized a high-level wireframe, displaying what such a tool could look like, and how measures could be included and categorized. Currently, five general categories have been proposed: State Medicaid Member Experience, Health Outcomes, Medicaid Program Actions, Demographics, and Underlying Factors. These would then be further stratified into varying numbers of domains, under which individual measures could be housed.
To begin a process as large in scope as populating such a data tool, SHADAC decided to narrow our focus and initially concentrate on one potential category area – Medicaid Member Experience. A variety of reasoning went into the decision to start with this category.
- First, since centering the Medicaid member has been, and continues to be, a pivotal focus of all MET project work, so, too, should attempting to understand and represent their experiences be at the center of our measurement data scan and tool population work. We also believe that these data would be the most important in understanding how meaningful these measures are to the Medicaid community members themselves.
- Second, because of SHADAC’s extensive background and familiarity working with a variety of federal surveys and other data sources that support state estimates, we knew where to begin in examining data availability and completeness for existing quantitative data.
After an extensive data and measurement scan focused on Medicaid member experience, SHADAC researchers have compiled their findings thus far into a new resource. This resource highlights a number of key data sources that hold the greatest potential for measuring population in this area, including the Behavioral Risk Factor Surveillance System (BRFSS), the National Survey of Children’s Health (NSCH), the Survey of Income and Program Participation (SIPP), the Pregnancy Risk Assessment Monitoring System (PRAMS), and National Core Indicators – Aging and Disabilities and National Core Indicators – Intellectual and Developmental Disabilities (NCI-AD/NCI-IDD).
Not only that, but this resource also points to critical gaps in availability and existence of data sources and data measures themselves, including highlighting the lack of data stratification for key demographic groups. The resource also details potential measures that would benefit such a tool but are not currently part of any known data collection efforts. Additionally, SHADAC researchers outline several proposals for addressing these gaps with suggested improvements for current data collection efforts/programs alongside proposals for new data collection methods.
Blog & News

Race/Ethnicity Data in CMS Medicaid (T-MSIS) Analytic Files: 2021 Data Assessment
December 6, 2023:The Transformed Medicaid Statistical Information System (T-MSIS) is the largest national database of current Medicaid and Children’s Health Insurance Program (CHIP) beneficiary information collected from U.S. states, territories, and the District of Columbia (DC).1 T-MSIS data are critical for monitoring and evaluating the utilization of Medicaid and CHIP, which together provide health insurance coverage to almost 90 million people.2
Due to their size and complexity, T-MSIS data files are challenging to use directly for research and analytic purposes. To optimize these files for health services research, Centers for Medicare and Medicaid Services (CMS) repackages them into a user-friendly, research-ready format called T-MSIS Analytic Files (TAF) Research Identifiable Files (RIF). One such file, the Annual Demographic and Eligibility (DE) file, contains race and ethnicity information for Medicaid and CHIP beneficiaries. This information is vital for assessing enrollment, access to services, and quality of care across racial and ethnic groups in the Medicaid/CHIP population, whose members are particularly vulnerable due to limited income, physical and cognitive disabilities, old age, complex medical conditions, housing insecurity, and other social, economic, behavioral, and health needs.
To guide researchers and other consumers in their use of T-MSIS data, CMS produces data quality assessments of the completeness of race and ethnicity data along with other data such as enrollment, claims, expenditures, and service use. The Data Quality (DQ) assessments for race and ethnicity data have been posted for data years 2014 through 2021 and indicate varying levels of “concern” regarding race and ethnicity data completeness. Some data years have multiple data versions (e.g., Preliminary, Release 1, Release 2), each with their own DQ assessment.
While completeness of race and ethnicity data reported to CMS has historically remained inconsistent among the states, territories, and DC, SHADAC has been monitoring the quality of these data over time. We are excited to discuss a noticeable improvement in quality as discussed below. This blog explores not only the 2021 Data Release 1, the most recent T-MSIS race and ethnicity data for which a DQ assessment is available, but also a brief analysis of data quality trends over time that we plan to follow in future T-MSIS file releases.
Evaluation of T-MSIS Race and Ethnicity Data
DQ assessments for each year and data version of T-MSIS data are housed in the Data Quality Atlas (DQ Atlas), an online evaluation tool developed as a companion to T-MSIS data.3 The DQ Atlas assesses T-MSIS race and ethnicity data using two criteria: the percentage of beneficiaries with missing race and/or ethnicity values in the TAF; and the number of race/ethnicity categories (out of five) that differ by more than ten percentage points between the TAF and American Community Survey (ACS) data. Taken together, these two criteria indicate the level of “concern” (i.e., reliability) for states’ T-MSIS race/ethnicity data. To construct the external ACS benchmark for evaluating T-MSIS data, creators of the DQ Atlas combine race and ethnicity categories in the ACS to mirror race and ethnicity categories reported in the TAF (see Table 1). More information about the evaluation of T-MSIS race and ethnicity data is available in the DQ Atlas’ Background and Methods Resource.
Five “concern” categories appear in the DQ Atlas: Low Concern, Medium Concern, High Concern, Unusable, and Unclassified. States with substantial missing race/ethnicity data or race/ethnicity data that are inconsistent with the ACS – a premier source of demographic data – are grouped into either the High Concern or Unusable categories, whereas states with relatively complete race/ethnicity data or race/ethnicity data that align with ACS estimates are grouped into either the Low Concern or Medium Concern categories. The Unclassified category includes states for which benchmark data are incomplete or unavailable for a given data year and version.
Table 1. Crosswalk of Race and Ethnicity Variables between the TAF and ACS
| Race/Ethnicity Category |
Race/Ethnicity Flag Value in TAF |
Combination of Race and Hispanic Variables in ACS |
| Hispanic, all races |
7=Hispanic, all races | Hispanic, all races |
| Other races, non-Hispanic |
4= American Indian and Alaska Native, non-Hispanic 5=Hawaiian/Pacific Islander 6=Multiracial, non-Hispanic |
- American Indian alone - Alaska Native alone - American Indian and Alaska Native tribes specified; or American Indian or Alaska native, non-specified and no other race - Native Hawaiian and other Pacific Islander alone - Some other race alone - Two or more races |
Source: Medicaid.gov. (n.d.). DQ Atlas: Background and methods resource [PDF file]. Available from https://www.medicaid.gov/dq-atlas/downloads/background-and-methods/TAF-DQ-Race-Ethnicity.pdf Accessed December 1, 2023.
Quality Assessment by State
Table 2 shows the Race and Ethnicity DQ Assessments for the 2021 TAF (Data Version: Release 1). The categorization criteria used to determine the levels of concern for the 2021 TAF Release 1 data are the same as those used to assess T-MSIS data from previous years and versions. 16 states received a rating of “Low Concern.” There were 22 states (including Puerto Rico [PR]) that fell into the “Medium Concern” category.
Most of the “Medium Concern” states (19 of 22) fell into the subcategory denoting the higher percentage range of missing race/ethnicity data (from 10 percent up to 20 percent). A similar pattern can be seen among the “High Concern” states, most of which (8 of 11) fell into the subcategory denoting the highest percentage range of missing race/ethnicity data (from 20 percent up to 50 percent).
Finally, 11 states (including DC) received a rating of “High Concern.” Three states (Massachusetts, Tennessee, and Utah) received an “Unusable” rating, as each of these states was missing at least 50 percent of race/ethnicity data. The Virgin Islands (VI) is the only state/territory categorized as “Unclassified” in the 2021 TAF (Data Version: Release 1) due to insufficient or incomplete data, and does not appear in Table 2.
Table 2. Race and Ethnicity Data Quality Assessment, 2021 T-MSIS Analytic File (TAF) Data Release 1
| Data quality assessment |
Percent of beneficiaries with missing race/ethnicity values | Number of race/ethnicity categories where TAF differs from ACS by more than 10% |
Number of states* |
States |
| Low Concern | <10% | 0 | 16 | AK, DE, GA, KS, MI, MO, NE, NV, NM, NC, ND, OH, OK, PA, SD, WA |
| Medium Concern | <10% | 1 or 2 | 3 | ID, IL, VA |
| 10% - <20% | 0 or 1 | 19 | AL, AR, CA, CO, FL, IN, KY, ME, MD, MN, MS, MT, NH, NJ, PR, TX, VT, WV, WI | |
| High Concern | <10% | 3 or more | 1 | RI |
| 10% - <20% | 2 or more | 2 | AZ, LA | |
| 20% - <50% | Any value | 8 | CT, DC, HI, IA, NY, OR, SC, WY | |
| Unusable | >50% | Any value | 3 | MA, TN, UT |
Notes: *T-MSIS includes all 50 states, the District of Columbia (DC), and the U.S. territories of Puerto Rico (PR) and the Virgin Islands (VI). However, a DQ assessment is not available for VI in the 2021 TAF (Data Version: Release 1) due to incomplete/unavailable data.
Despite ongoing variation in the completeness of race and ethnicity data reported to CMS, SHADAC researchers have noted a trend toward better quality data overall. Since beginning to track these quality assessments with the 2019 T-MSIS TAF release, a number of states have shifted up the quality assessment scale with noticeably fewer states seeing their data classified as “High Concern.” Specifically, 2021 race/ethnicity TAF data from 11 states received a rating of “High Concern” compared to 16 states’ data in 2020 and 17 states’ data in 2019. The number of states with “Unusable” data has also dropped each year – 3 states’ 2021 race/ethnicity TAF data was classified as “Unusable” compared to 4 states’ data in 2020 and 5 states’ data in 2019.
Visualizing T-MSIS Data in the DQ Atlas
The DQ Atlas enables users to generate maps and tables that compare the quality of T-MSIS data between states across different topics, such as race/ethnicity, age, income, and gender (see Figure 1). Visualizing T-MSIS data in this manner can help researchers quickly assess the completeness of a single variable as well as the relative completeness (or incompleteness) of certain variables compared to others. For example, in the 2021 TAF Data Release 1, all states and territories received a “Low Concern” rating for age data, whereas only 31 states and territories received a “Low Concern” rating for family income.
Figure 1. Data Quality Assessments of Beneficiary Information by U.S. State/Territory

Notes: Green = low concern; yellow = medium concern; orange = high concern; red = unusable; grey = unclassified.
Source: Medicaid.gov. (n.d.). DQ Atlas: Race and Ethnicity [2021 Data set: Version: Release 1]. Available from https://www.medicaid.gov/dq-atlas/landing/topics/single/map?topic=g3m16&tafVersionId=35 Accessed December 1, 2023.
Looking Ahead
Increasingly, a wide diversity of voices from non-profits, health insurers, state-based marketplaces, and policymakers have called for improving the collection of race, ethnicity, and language data, often with the goal of advancing health equity. CMS’s efforts to improve the quality and availability of T-MSIS data reflect this nationwide movement toward data collection practices that more accurately capture the diversity of the U.S. population.
SHADAC was excited to see the revised Office of Management and Budget (OMB) standards related to the collection of race and ethnicity data. The proposed revisions align with available evidence, are consistent with the changes made by leading states, and, most importantly, explicitly state that these standards should serve as a minimum baseline with a call to collect and provide more granular data. However, while these standards are specifically named as minimum reporting categories for data collection throughout the Federal Government, if adopted they are likely to shape data collection and reporting across all sectors, including the states that collect race/ethnicity data through the Medicaid application process.
Many states express difficulties reporting data, as there is misalignment in how state eligibility systems, Medicaid Management Information System (MMIS), and T-MSIS format race and ethnicity data. Before states submit data to T-MSIS, they must reformat and aggregate data, which may affect the quality of submitted data. One approach to improve the collection and reporting of data is providing states with an updated model application using evidence-based approaches to race and ethnicity questions that improve applicant response rate and data accuracy.
Sources
1 Medicaid.gov. Transformed Medicaid Statistical Information System (T-MSIS). Retrieved October 20, 2022, from https://www.medicaid.gov/medicaid/data-systems/macbis/transformed-medicaid-statistical-information-system-t-msis/index.html#
2 Medicaid.gov. August 2023 Medicaid & CHIP Enrollment Data Highlights. Retrieved on December 1, 2023, from https://www.medicaid.gov/medicaid/program-information/medicaid-and-chip-enrollment-data/report-highlights/index.html3 Saunders, H., & Chidambaram, P. (April 28, 2022). Medicaid Administrative Data: Challenges with Race, Ethnicity, and Other Demographic Variables. Kaiser Family Foundation. Retrieved October 31, 2022, from https://www.kff.org/medicaid/issue-brief/medicaid-administrative-data-challenges-with-race-ethnicity-and-other-demographic-variables/
4 Wang, H.L. (June 15, 2022). Biden officials may change how the U.S. defines racial and ethnic groups by 2024. NPR. Retrieved November 1, 2022, from https://www.npr.org/2022/06/15/1105104863/racial-ethnic-categories-omb-directive-15
5 Diaz, J. (August 16, 2022). California becomes the first state to break down Black employee data by lineage. NPR. Retrieved November 1, 2022, from https://www.npr.org/2022/08/16/1117631210/california-becomes-the-first-state-to-break-down-black-employee-data-by-lineage
6 The New York State Senate. (December 22, 2021). Assembly Bill A6896A. Retrieved November 2, 2022, from https://www.nysenate.gov/legislation/bills/2021/A689

