 VISIT STATE HEALTH COMPARE
VISIT STATE HEALTH COMPARE
Blog & News





Minnesota's 2018 Preliminary Individual Market Premium Rate Filings in Context: News Is Good but Challenges Remain
August 21, 2017:From the Desk of Lynn Blewett
Minnesota insurance companies filed their preliminary premium rates for plans sold on the individual health insurance market. The rate increases for 2018 are much lower than the rate increases seen last year when premiums increases were as high as 50 to 67 percent. This blog provides my initial impressions on the preliminary rate increases for 2018 and additional context to understand the dynamics of a rapidly evolving health insurance market.
Minnesota’s individual health insurance market is in a state of flux with the implementation of the Affordable Care Act (ACA). Individuals without access to employer-sponsored insurance and without access to the premium subsidies offered through MNsure faced exorbitant, and for some, unaffordable, health insurance premiums in 2016. This crisis prompted the Minnesota legislature to pass two pieces of significant legislation last session. The Health Insurance Premium Relief bill provided enrollees with rebates to health plans, with the requirement that quoted premium prices would be reduced by 25%. The Premium Security Plan established a reinsurance plan to provide additional premium relief and stabilize the premiums in the individual market. Together, the legislature authorized nearly $1 billion in support of the individual health insurance market.
Rate Increases with and without Reinsurance
The rate increases for 2018 are presented in the table below. Rate increases with reinsurance ranged from a 14.5 percent decrease in premiums submitted by UCare to an 11.4 percent increase in rates submitted by Blue Plus. Without reinsurance, the rate increases ranged from a 3.3 percent increase in rates submitted by Group Health to a 31.7 percent increase submitted by Blue Plus.
| Proposed 2018 Individual Market Health Insurance Rates for Minnesota | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Insurer |
Proposed Average Change with Reinsurance |
Proposed Average Change without Reinsurance |
|||||||||
| Blue Plus | -1.5% | to | +11.4% | +16.4% | to | +31.7% | |||||
| Group Health* | -14.5% | to | -13.4% | +3.3% | to | +4.6% | |||||
| Medica Insurance Company* | -5.3% | to | +5.3% | +15.4% | to | +29.4% | |||||
| PreferredOne Insurance Company^ | -40.8% | to | -36.8% | -25.5% | to | -20.6% | |||||
| UCare | -14.5% | +9.4% | |||||||||
| *Current HealthPartners Insurance Company enrollees will default renew into Group Health, and current Medica Health Plans of Wisconsin enrollees will default renew into Medica Insurance Company. A consumer is not required to accept the default renewal plan and may select any plan from any insurer during open enrollment. | |||||||||||
| ^PreferredOne Insurance Compnay left the Minnesota individual market in 2015 and is not offering new insurance products. | |||||||||||
| Source: 2018 Proposed Health Insurance Rates,” Minnesota Department of Commerce, July 31, 2017. | |||||||||||
| State 1332 Innovation Waivers | ||
|---|---|---|
|
Section 1332 of the Affordable Care Act provides the opportunity for states to propose innovative strategies around the access expansions included in the ACA—including the Medicaid expansion and the premium subsidies provided through tax credit for those buying on the exchange within certain income limits. The plans must be approved by both the Secretary of Health and Human Services and by the Department of the Treasury; must provide at least the level of coverage provided under the ACA; and may not increase the federal deficit. The waivers are approved for five-year periods. State-based reinsurance represents one of the first policy strategies being implemented to stabilize the individual market. Reinsurance also represents a key policy strategy of interest to CMS as evidenced by a March 13, 2017 communication from HHS Secretary Price, sent to each Governor, encouraging states to consider using the 1332 waiver opportunity to implement reinsurance programs and making specific reference to the Alaska reinsurance approach. Alaska's Reinsurance Approach Alaska’s 1332 waiver proposal to establish a reinsurance program was recently approved by the federal government. Alaska’s reinsurance plan is financed through assessments on private health insurers with additional federal funding of $332 million over a five-year period. Alaska uses a condition-specific reinsurance approach that provides 100 percent of the cost of all claims for policyholders that have one of 33 pre-existing conditions. Pass-Through Funding Alaska's waiver, and Minnesota's waiver proposal, uses “pass through” federal dollars—funding that otherwise would be used for the subsidies offered on the Health Insurance Marketplace, namely the Advanced Premium Tax Credits (APTC) and the Consumer Cost-Sharing Reductions (CSRs). Because premiums are expected to go down under reinsurance, the subsidies required to fund the APTCs and the CSRs would be reduced, and the amount of savings from reduced subsidies would be “passed through” to the state to help fund its reinsurance program. Each state must estimate the amount of federal savings achieved through reinsurance and include this in its waiver application. |
Minnesota’s Reinsurance Proposal
Insurance companies buy reinsurance to reduce the volatility in their costs and provide stability to premiums. Reinsurance is basically insurance for insurance companies and is standard practice for different types of insurance products, not just health care. There are different models of reinsurance, and Minnesota is one of five states with current reinsurance proposals for health insurance offered in the individual market.
Minnesota proposed a publicly-funded reinsurance program using a claims corridor approach. The reinsurance company will reimburse insurers at an 80%/20% coinsurance rate for claims that fall between $50,000 and $250,000. Instead of the insurers covering the costs of reinsurance, the state has proposed public financing with an appropriation of $271 million per year for two years—a total of $542 million for the biennium.
The legislatively-created Minnesota Comprehensive Health Association would serve as the administrator of the reinsurance product, using state funds appropriated to the commissioner of commerce. The legislative language authorizing the reinsurance program requires federal approval of a State Innovation Waiver (a 1332 waiver), which was submitted on May 5, 2017. Under this waiver, Minnesota has proposed that the federal government pay about a third of the cost of the reinsurance program, with tthe federal government contributing between $138 million and $167 million toward the $270 million total cost of the program each year.
My Initial Thoughts
In general, the 2018 preliminary insurance rate filings are great news. Minnesota’s individual market is relatively small (about 300,000 pre-ACA and 170,000 in 2017), and implementing insurance reforms was difficult. The premiums in the individual market started low but over time had to catch up with increases in costs. Many of the premiums filed last year increased by more than 50% from 2016. The first look at the preliminary 2018 rates with limited increases, and in some cases decreases, was welcome.
There is also some hope that Secretary Price will approve Minnesota’s 1332 State Innovation Waiver. He recently approved the waiver proposal submitted by the state of Alaska, and the Minnesota approach to reinsurance is relatively straightforward. Governor Dayton recently met with Secretary Price, and the meeting reportedly went well.
However, there continues to be uncertainty at the federal level in terms of conflicting messaging around federal funding of CSRs and enforcement of the individual mandate, and the broader political debate about the ACA’s future has further escalated insurers’ concerns. These factors, in turn, have led to the exit of insurers from local markets or entire states, exceedingly high increases in premiums, and fewer plan choices for consumers.
Here are a few of my initial concerns.
- The legislature funded reinsurance for just two years, and reinsurance is likely to be an ongoing need. The state appropriated funding for just two years using funds from the Health Care Access Fund. If state-based reinsurance will be an ongoing need, and I suspect it will, a new source of funds will need to be found.
- Financing of reinsurance uses funding from Minnesota's Health Care Access Fund (HCAF), which may soon be needed to support the state's safety net. Typically, reinsurance is funded by assessments on private insurers to cede a portion of their risk to another insurance company. The temporary reinsurance program provided in the ACA and the more recent Alaska reinsurance program were both funded with assessments on the insurance carriers.
The HCAF comes from a two percent fee on most health care providers’ bills. The HCAF was initially established to fund MinnesotaCare, which was designed to support health insurance coverage for Minnesotans whose incomes fell just above the Medicaid income limits. The target population was Minnesota families working in low-wage jobs with no access to employer-based health insurance. MinnesotaCare provided needed coverage and limited premiums based on income, and providers who once provided care without payment now received reimbursement for their services.
Minnesota was fortunate to move into the 2017 legislative session with a $1.6 billion dollar surplus, allowing the legislature to fund different programs including the premium rebates described above. Yet given the uncertainty at the federal level and discussions of cuts to safety net programs such as Medicaid, the HCAF may be needed in the near future to support the safety net in Minnesota as initially intended. For long-term funding of reinsurance, alternative financing should be considered, including fees assessed on the insurance carriers.
- The 105,000 people purchasing coverage on MNsure who got a 25 percent rebate on their premiums this year will likely see some increase in their premiums next year, even with reinsurance. The premium increases cited in the table above are based on last year’s base premiums without the 25 percent premium rebate adjustment. For example, a person facing a $1,000 a month premium in 2017 received a 25 percent rebate, bringing their 2017 premium to $750. But even with no premium increase for 2018, the individual would be back to the $1,000 premium, which represents a 33% increase.
In general, rates will remain flat for most people who purchase coverage on Minnesota's health insurance exchange, MNsure: Premium increases will not be felt by the 85 percent of people who are income-eligible (i.e., with an income of $24,000 to $48,680 annually for a family of four) for Advanced Premium Tax Credit subsidies to bring down the cost of their monthly premiums: Because the amount of the subsidy is based on household income, such that no individual will pay more than 9.6 percent of income on health insurance premiums, premium rate increases are absorbed by the premium subsidy. However, broad premium decreases for this segment of the MNsure population won't happen, either.
- We still do not know if every Minnesota county will have options to purchase coverage in the individual market. And we do not know what the provider networks look like. Last year, the networks were tighter, and some of the pairings of hospitals and clinics did not facilitate the best geographical access. So, we still need to see what the plans look like and if all counties are covered.
- The PreferredOne products with the largest declines in premiums are not offered on Minnesota's individual market for new enrollees. These are the products that have retained enrollees since PreferredOne abruptly left the individual market in 2015. They are not offering new products.Technically, PreferredOne should not be included on this list because its products are not currently offered on the individual market.
States like Minnesota and Alaska are forging ahead and making decisions to assure that people have access to affordable coverage. We are out in front of the pack but still have work to do.
Blog & News

HHS Approves Alaska's 1332 State Innovation Waiver for State-Based Reinsurance
July 12, 2017: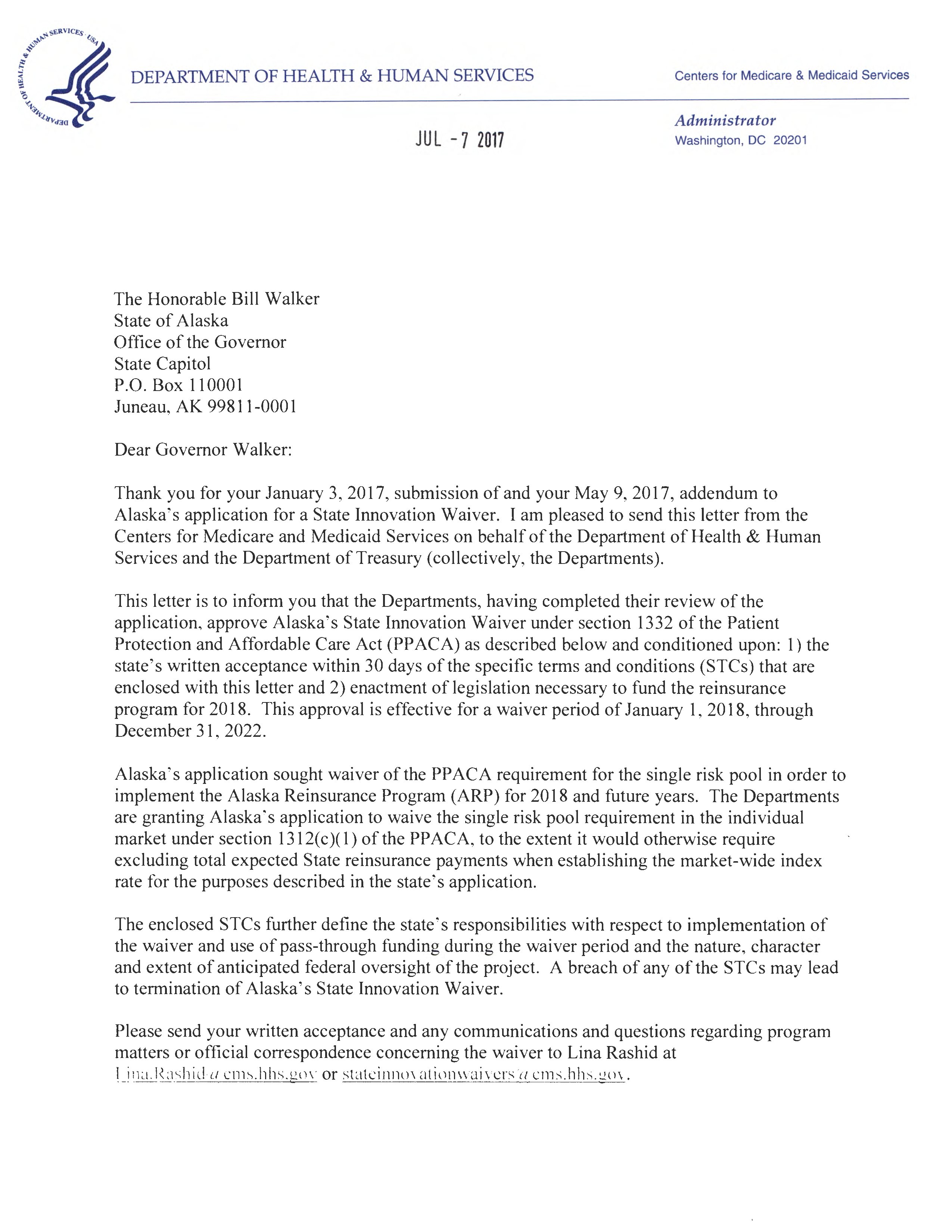 On July 7, 2017, the U.S. Department of Human Services, along with the Department of the Treasury, approved Alaska's 1332 Waiver proposal seeking federal funding of its state-based reinsurance proposal. The state was awarded $48.3 million in federal pass-through funding in 2018 and a total of $322 million over five years. This is the first such waiver that has been approved to date, with two more--from Minneosta and Iowa--under review.
On July 7, 2017, the U.S. Department of Human Services, along with the Department of the Treasury, approved Alaska's 1332 Waiver proposal seeking federal funding of its state-based reinsurance proposal. The state was awarded $48.3 million in federal pass-through funding in 2018 and a total of $322 million over five years. This is the first such waiver that has been approved to date, with two more--from Minneosta and Iowa--under review.
SHADAC is tracking state reinsurance proposals as they are submitted and reviewed by HHS, and we have updated our blog with details that reflect this newest development.
Blog & News
Google Trends: A Rich Source of Data for Health Policy Analysis - New Brief
May 30, 2017: A new brief from SHADAC examines Google Trends as a source of internet search data and provides an example of how researchers are using these data to study health policy under a grant from the Robert Wood Johnson Foundation (RWJF) SHARE program.
A new brief from SHADAC examines Google Trends as a source of internet search data and provides an example of how researchers are using these data to study health policy under a grant from the Robert Wood Johnson Foundation (RWJF) SHARE program.
The brief authors note that the data available through Google Trends can be used to study health policy at both the state and sub-state level over time and offer some advantages over traditional sources of surveillance data (e.g., surveys) including timeliness, efficiency, transparency, and accessibility. However, users should be aware that certain groups of people might be over- or under-represented among internet search data because of variability in online access and internet search usage among subpopulations. Additionally, there is some evidence that Google Trends search results are not stable over time due to continuous algorithm updates by Google.
The brief highlights the use of Google Trends by Dr. Sarah Gollust (University of Minnesota) and Dr. Erika Franklin Fowler (Wesleyan University), who capitalized on the data available through Google Trends in order to conduct a SHARE-funded analysis of (a) whether geographic regions with higher rates of uninsurance spent more time researching ACA marketplace plans and health insurance coverage generally during the first ACA open enrollment period and (b) whether other local-level factors were associated with higher search volumes. The researchers found that internet searches for health insurance terms varied widely across the country, with areas of high pre-ACA rates of uninsurance more likely to search in higher volumes for the key terms "Obamacare" and "health insurance," and geographically dispersed rural areas exhibiting a higher search volume than large urban areas.
Learn more about the SHARE project led by Sarah Gollust and Erika Franklin Fowler.
About SHARE
State Health Access Reform Evaluation (SHARE) is a national program of the Robert Wood Johnson Foundation that supports rigorous research on issues surrounding state health reform. The SHARE program is managed by SHADAC.
Publication
Using Google Trends to Support Health Policy Analysis
This brief describes a rich source of internet search data--Google Trends--and provides an example of how researchers are using these data to study health policy.
Access additional content from the SHARE-funded research project led by Dr. Sarah Gollust and Dr. Erika Franklin Fowler.
Publication
Virtual Tour of State Health Compare (Webinar)
May 23, 2017, at 12:00 p.m. Central / 1:00 p.m. Eastern
On May 23rd, SHADAC hosted a virtual tour of State Health Compare, a new, user-friendly online tool for obtaining and comparing state-level estimates related to health and health care.
![]() State Health Compare: How's It Different?
State Health Compare: How's It Different?
State Health Compare combines estimates previously available separately through the SHADAC Data Center and the Robert Wood Johnson Foundation (RWJF) Data Hub. The new, merged tool brings together estimates on a wide range of health-related topics in an effort to allow analysts and policymakers to view state-level data through a broad Culture of Health lens.
The Virtual Tour: What Will You Learn?
SHADAC Senior Research Fellow Joanna Turner guided attendees on a tour of State Health Compare's user interface. Ms. Turner provided an overview of available estimates and showed how users can generate maps, bar charts, trend lines, and tables to examine the estimates within and across states and over time, as well as by characteristics such as age, race/ethnicity, etc. Attendees also learned how to download graphics and export the underlying data.
Ms. Turner was joined on the webinar by Carolyn Miller, Senior Program Officer at RWJF, and by SHADAC Director Lynn Blewett. SHADAC Senior Research Fellow Brett Fried will also be available to answer questions.
View the presentation slides here or watch the recording below.
View the event transcript here.
Related Resources
Hest, R. (2017). "Significance Testing Using State Health Compare." SHADAC Technical Brief. Minneapolis, MN: State Health Access Data Assistance Center.
SHADAC. (2013). "Using SHADAC Health Insurance Unit (HIU ) and Federal Poverty Guideline (FPG) Microdata Variables." SHADAC Technical Brief.Minneapolis, MN: State Health Access Data Assistance Center.
SHADAC. (2011). "FPG vs. FPL: What's the Difference?" SHADAC Blog. Minneapolis, MN: State Health Access Data Assistance Center.

