SHADAC’s State Health Compare is an online data visualization tool that allows users to explore and download health data sets and statistics. These data are broken down into measures that range from ‘Insurance Coverage Type’ to ‘Suicide Deaths’; measures are divided into overall categories like “Health Behaviors”, “Cost of Care”, “Health Outcomes”, and more.
SHADAC’s public health research fellows and analysts consistently update measures on State Health Compare (SHC) in order to provide users with the most up-to-data available data. In this post, we will review the health data sets and measures that have been updated since our last measure update blog, including a short explanation of the measure and its data source.
Updates Using DEA and CDC Data
The Drug Enforcement Administration (DEA) provides data on transactions of controlled substances provided by manufacturers and distributors via their ARCOS system (Automated Reports and Consolidated Ordering System). Using this data, we updated the following measure on SHC:
The opioid epidemic in the United States has been an ongoing public health issue dating back to the mid- to late-90s and early 00s, with many attributing overprescription of opioid painkillers (and resulting drug dependence) as one of the catalysts to the epidemic. Tracking sales of prescription opioids can be a useful tool for understanding prescription opioid use over time, the potential source of opioids being used (e.g., prescription, illicit drugs like fentanyl, etc.), and geographical areas that may be more susceptible to opioid-related health effects or overdoses.
This measure provides data on prescription opioid painkiller sales in kilograms per 100,000 people by state and nationally. Specifically, this measure tracks sales of oxycodone and hydrocodone (brand names Vicodin and Oxycontin). Estimates are available by year, from 2000 through 2023.
Updates Using CDC WONDER
Via the CDC WONDER (Wide-ranging ONline Data for Epidemiologic Research) database using National Vital Statistics System (NVSS) data, SHADAC researchers updated the following measures:
Opioid-Related and Other Drug Poisoning Deaths
Thousands of people in the U.S. die each year due to drug overdoses – monitoring rates of drug overdose deaths, and what drugs were attributed to those deaths, can help us understand what substances are causing the highest numbers of deaths over time. State Health Compare also allows users to see geographic differences, allowing for more targeted initiatives and policy development to hopefully reduce the number of drug poisoning deaths.
This measure provides data on opioid-related and other drug poisoning deaths per 100,000 people by state and nationally. Estimates are available by year, from 1999 through 2022.
Related Blog: “During the Pandemic, Drug Overdoses Became the Third Leading Cause of Death for U.S. Adolescents”
Along with drug-related deaths, alcohol-involved deaths continue to account for thousands of deaths annually. In fact, alcohol-involved deaths are among the top causes of preventable deaths in the U.S. This includes deaths from a variety of alcohol-related causes, like alcoholic liver disease, alcoholic gastritis, accidental poisoning, and more.
Specifically, the SHC measure provides data on alcohol involved deaths by state and nationally per 100,000 people. Estimates are available by year, from 1999 through 2022.
Concerningly, a recent publication from SHADAC found an acceleration of alcohol-attributable deaths across the U.S. during the pandemic. Learn more in the full “Sobering Statistics” brief on alcohol-attributable deaths.
CDC WONDER data also allowed us to update SHC’s Suicide Deaths measure, providing estimates of suicide deaths per 100,000 people by state and by year, from 1999 to 2022. This measure also allows users to break down estimates by age, sex, race/ethnicity, metropolitan status, and use of a firearm.
Update Using Bureau of Labor Statistics (BLS) Data
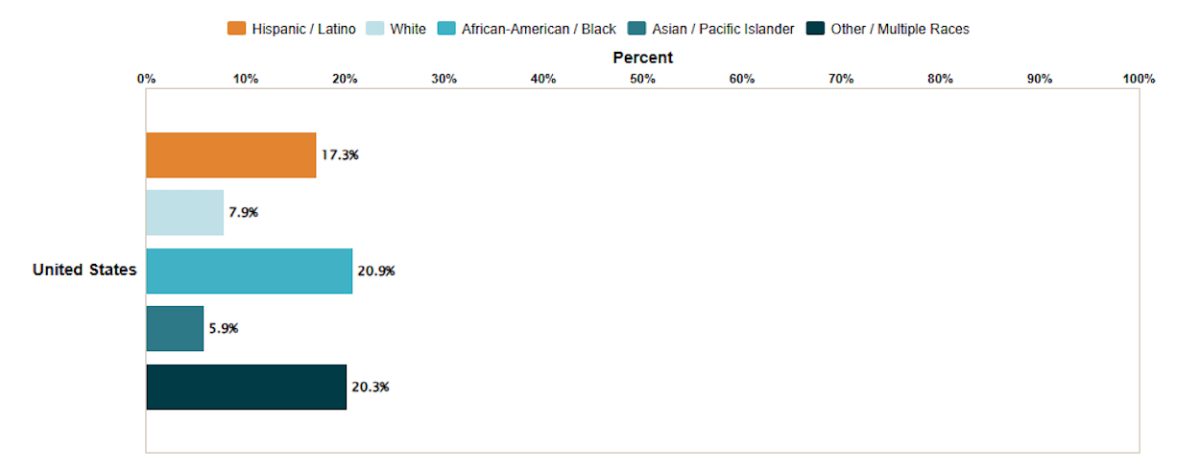
Previously, SHADAC added an ‘Unemployment Rate’ measure to State Health Compare using Bureau of Labor Statistics (BLS) data with state-level and national data available for each year from 2000 through 2023.
In July 2024, we were able to expand this measure to disaggregate by race/ethnicity (Hispanic / Latino, African-American / Black, Asian, and White), allowing users to better understand any racial disparities in unemployment.
This blog can help you learn more about unemployment rate trends of the past 5-years (pre-, mid-, and post-pandemic).
Updates Using TFAH, CDC, and MEPS Survey Data
The Medical Expenditure Panel Survey (MEPS) is a national survey on health care use, cost, and quality. SHADAC uses MEPS survey data (specifically from the Insurance/Employer Component) to populate and update the following measures related to Employer Sponsored Insurance (ESI) on State Health Compare:
Workers in Establishments that Offer Coverage
Employee Contributions to Premiums (percent of annual premiums contributed by employees)
High-Deductible Health Plans (percent of private-sector employees enrolled in high-deductible health insurance plans)
With ESI still the number one source of health insurance coverage for the majority of Americans, SHC’s ESI measures allow researchers and policymakers to better understand and evaluate access and affordability of this important coverage source.
Learn more about ESI in the post-pandemic U.S. in this SHADAC brief.
We updated this measure using data from the National Center for Injury Prevention and Control (NCIPC) using the CDC WISQARS database. Premature deaths (defined as deaths that occur before the population’s average age of death) are often unintentional and/or violence related, and include deaths from vehicle crashes, homicide, drug overdoses, lifestyle-related injuries/illnesses, and more.
Specifically, this measure reports the average number of years of potential life lost prior to age 75 per 100,000 people. This measure can be broken down by race/ethnicity and by year from 2000 through 2022.
Using data collected by Trust for America’s Health (TFAH), we also updated our Public Health Funding measure that reports the dollar amount per person allocated for public health funding by state.
Update Using American Community Survey and Current Population Survey Data
The American Community Survey and the Current Population Survey are both large-scale federal survey resources, gathering data on health insurance coverage, demographic data collection, employment information, and more. While similar, there are key differences between the ACS vs CPS that we delve into in a previous blog.
We updated our ‘Income Inequality’ measure using the Gini Coefficient from the ACS. The Gini Coefficient ranges between 0 and 1 – a higher Gini Coefficient value indicates more income inequality (0 indicates perfect equality and 1 indicates perfect inequality). This measure allows users to see disparities in income distribution between states and compare to the national Gini Coefficient value; this measure is available for years 2006 through 2023.
We also updated the following measures using the ACS:
We also used the CPS to add a new measure:
This new measure was using the Current Population Survey Food Security Supplement. Research has shown that food insecurity, aka having limited or unstable access to food, is linked to poorer health outcomes, higher chronic disease prevalence, and overall financial hardship.
This measure is defined as, "Percentage of households that have experienced food insecurity (i.e. low or very low food security)." It is available for four different time frames at both the state-level and nationally. We have also added two breakdowns: by race/ethnicity and by presence of child in household.
Curious how those factors could impact food insecurity rates? Check out this blog on food insecurity in America that delves into this measure and its breakdowns.
After adding a new measure using the Current Population Survey, we were able to update a number of our other measures that use CPS data:
People with High Medical Care Cost Burden
Medical Out-of-Pocket Spending
Update Using BRFSS Data
The Behavioral Risk Factor Surveillance System (BRFSS) is an annual, telephone-based survey of U.S. adults that collects data on health-related questions including demographic information, behaviors, perceptions, and more.
BRFSS data includes 50-state data on health outcomes and behaviors, giving researchers and analysts a helpful resource for tracking the effects of health policy and initiatives.
Learn more about what the BRFSS is and how researchers can use it here.
Using BRFSS data, we updated the following measures:
Adults Who Forgo Needed Medical Care Due to Cost
Adult Excessive Alcohol Consumption
Activities Limited Due to Health Difficulty
Adults with No Personal Doctor
Also using the BRFSS, we added a brand-new measure:
SHADAC follows emerging public health and health policy trends in order to provide users with relevant and timely information. This measure provides a state-level look at the percentage of the adult population who have a condition that could result in them being denied health insurance coverage if protections under the Affordable Care Act were overturned.
Final 2024 Updates
Finally, we updated the following measures:
Medicaid Expenses as a Percent of State Budgets - using data from National Association of State Budget Officers (NASBO)
Child Vaccinations – using data from the National Immunization Surveys (NIS)
Explore Up-to-Date Data Visualizations, Health Statistics, and Health Data Sets on State Health Compare
All of these measures, and more, are available now on State Health Compare. You can explore the state-level data and health statistics yourself, creating customized data visualizations and downloadable health data sets for your own analysis.
Have you used State Health Compare for a project, report, publication, or blog? We would love to hear from you! Contact us here, or you can follow and tag us on LinkedIn.