Blog & News
Walsh, Elliot
Hest, Robert
Lukanen, Elizabeth




What Do the New Census Data Say About Insurance Coverage for Children and Adults? A Look at Both the National and State Level (SHVS Cross-Post)
November 01, 2024:
The following Expert Perspective (EP) is cross-posted from State Health & Value Strategies.
Authors: Elizabeth Lukanen, Elliot Walsh, Robert Hest, SHADAC
Original posting date October 30, 2024. Find the original post here on the SHVS website.
Background on Census Data
Every fall, the U.S. Census Bureau releases detailed data on the population, including data on health insurance coverage. The American Community Survey (ACS) is the premier source for detailed state and substate data on income, poverty, disability, marital status, education, occupation, travel to work, disability, and health insurance coverage, among other topics. An important feature of the ACS is that it includes a large enough sample for estimates for all 50 states and the District of Columbia and, in most states, there is sample to explore data disaggregated by insurance coverage type, age, race/ethnicity, and more.
2023 Data Do Not Capture the Full Impact of Coverage Changes Related to Medicaid Unwinding
The new, full-year 2023 insurance estimates from the ACS reflect data collected from January 1, 2023 to December 31, 2023. This health insurance coverage data provide new national- and state-level insurance coverage estimates, but do not fully reflect the Medicaid unwinding.
According to administrative data from the Centers for Medicare & Medicaid Services, Medicaid and Children’s Health Insurance Program (CHIP) enrollment declined by 13.9 million between March 2023 and June 2024. Some of those who disenrolled likely transitioned to other coverage, and others may have become uninsured. However, coverage transitions that happened in 2024 are not captured in the 2023 estimates from the Census Bureau. Because of the large changes in Medicaid and CHIP coverage during the unwinding, compared to the current, on-the-ground reality in 2024, these 2023 coverage estimates likely overestimate rates of public coverage and potentially underestimate rates of uninsurance.
Despite this limitation, the data are still instructive about changes to coverage during the early months of the unwinding period and generally for the year 2023. This expert perspective looks at health insurance coverage estimates at the national and state levels, and examines children’s health insurance coverage, looking at children’s uninsurance rates by state and by income level. As more data are released SHADAC will conduct additional analyses, presenting coverage estimates across key demographic categories, including by race/ethnicity. Disaggregating data is critical to identifying inequities and gaps in coverage, informing policies to improve equity and to prevent new disparities. It is also vital for identifying state policies and practices effective in maintaining coverage for specific populations so that they might be adopted in other states.
Overall Uninsurance Rates Were Fairly Stable
The uninsurance rate in the U.S. remained unchanged from the previous year, sitting at 7.9% in 2023. This was mirrored by stability in uninsurance in the states. From 2022 to 2023, the uninsured rate fell in 11 states and increased in three states – Iowa, New Jersey, and New Mexico (these changes were statistically significant). Table 1 below highlights the states with the highest and lowest rates of uninsurance in 2023.
Table 1. States with the Highest and Lowest Rates of Uninsurance, 2023
|
Highest Rates of Uninsurance |
Lowest Rates of Uninsurance |
||
|---|---|---|---|
|
Texas |
16.4% |
Massachusetts |
2.6% |
|
Georgia and Oklahoma |
11.4% |
District of Columbia |
2.7% |
|
Nevada |
10.8% |
Hawaii |
3.2% |
|
Wyoming and Florida |
10.7% |
Vermont |
3.4% |
|
Alaska |
10.4% |
Minnesota |
4.2% |
Source: SHADAC analysis of U.S. Census Bureau 2022 and 2023 American Community Surveys. Click here for data from all states.
Children’s Uninsurance Rates Increased
Notably, while the overall uninsurance rate remained stable between 2022 and 2023, the rate for children went up slightly (rising from 5.1% in 2022 to 5.4% in 2023). This comes after two years of falling rates of uninsurance for kids.
Five states saw an increase in their uninsured rate for children (Alabama, Louisiana, New Mexico, South Carolina, and Texas). This wasn’t clearly driven by changes in private or public coverage, though, as both remained stable nationally and went up and down in a variety of states.
Texas is the only state where the data tell a clear story — there was a decline in public coverage for children (1.9 percentage point (PP) decrease to 36.8% in 2023) and an increase in uninsurance for children (1.0 PP increase to 11.9%).
Insurance Coverage Changes for Children (Birth Through Age 18), 2022 to 2023
Source: SHADAC analysis of U.S. Census Bureau 2022 and 2023 American Community Surveys.
Low-Income Children Saw Declines in Public Coverage
For U.S. children below 200% of the Census poverty threshold, uninsured rates rose by 0.4 PP to 7.3% in 2023 (see Figure 1 below). This significant increase was likely driven by a 0.6PP decrease in public coverage (bringing that national rate down to 72.6% in 2023) and a statistically unchanged rate of private coverage (27.0%).

Note: Low income children are defined as those below 200% of the Census poverty threshold. Source: SHADAC analysis of U.S. Census Bureau 2022 and 2023 American Community Surveys.
Among the states, Louisiana (+1.5PP), Michigan (+1.2PP), South Carolina (+1.6PP), and Texas (+1.5PP) all saw significant increases in uninsurance for low-income children, rising to 5.5%, 4.3%, 8.0%, and 15.4%, respectively. No states saw decreases in uninsurance rates for low-income children.
These increases in children without coverage are likely tied to declines in public coverage for low-income children. For example, Michigan saw a 3.1PP decrease in public coverage, bringing it down to 73.2%, and Texas saw a 2.5PP decrease in public coverage, bringing it down to 65.0%.
Health Equity Implications
Rising uninsurance rates for children, particularly for low-income children, has a number of implications for health equity. First, it is important to address the likely reason that uninsurance rates for low-income children rose. While the ACS data doesn’t collect information on the reasons for coverage transitions, the data suggests this was driven by declines in public coverage that correspond with the end of the Medicaid continuous coverage requirement (this is supported by administrative data showing that more than 4.5 million children lost Medicaid or CHIP between March 2023 and June 2024, a reduction of almost 11%).
Second, the essential role Medicaid plays in providing health insurance to low-income children, the majority of whom are racial and ethnic minorities, must be acknowledged. Over 60% of children enrolled in Medicaid and CHIP identify as African American or Black, Hispanic, Asian American, Native Hawaiian and Other Pacific Islander, American Indian or Alaska Native, or multi-racial (State Health Compare, SHADAC, University of Minnesota, Accessed 10/10/2024). Declines in public coverage therefore disproportionately impact children of color. This is supported by early evidence that enrollees who identified as Hispanic or Black were twice as likely to report losing coverage because they could not complete the renewal process. SHVS will explore differences in coverage losses by race and ethnicity as more data are released.
Finally, Medicaid plays a critical role in children’s ability to access care – children with Medicaid or CHIP coverage report high rates of having a usual source of care and access to routine care. Further, evidence shows that they were as likely in the past 12 months to have seen a doctor, had a well child visit, and have had a dental exam as privately insured children. While having Medicaid does not erase the health inequity propagated by systemic racism it does improve access to important healthcare services and losing that coverage risks widening gaps in equity. As stated earlier, the full impact of the unwinding isn’t reflected in the latest data as it only includes the beginning months of the unwinding period. It will be important to revisit this once data from the entire unwinding period is released in order to get the full picture of coverage changes for this and other groups.
Blog & News
Lukanen, Elizabeth
Zylla, Emily
Unwinding Ends, but States’ Reporting of Medicaid Renewal Data Continues (SHVS Cross-Post)
October 29, 2024:
The following Expert Perspective (EP) is cross-posted from State Health & Value Strategies. Authors: Emily Zylla and Elizabeth Lukanen, SHADAC
Original posting date August 13, 2024. Find the original post here on the SHVS website.
States have resumed their regular processes for renewing individuals’ Medicaid and Children’s Health Insurance Program (CHIP) coverage due to the end of the continuous coverage requirement set in place during the COVID-19 pandemic. During this unwinding period, advocates, policymakers, and the media have been keenly interested in understanding how this work has impacted coverage for Medicaid enrollees.
One key source of data has been the monthly Unwinding Data Reports that state Medicaid agencies were required to submit to the Centers for Medicare & Medicaid Services (CMS). These reports include indicators about activities related to eligibility renewals, call center operations, and transitions to Marketplace coverage; CMS began publicly reporting monthly snapshots of these data in August 2023. However, well before the federal government began reporting this unwinding data, many states began publishing their own state dashboards, publicly detailing their progress in restarting renewals.
The public release of renewal data, at both the federal and state level, has proven to be a valuable tool in understanding who lost Medicaid coverage and why during the unwinding. States have successfully used the data to both monitor renewal outcomes and adjust outreach and administrative enrollment policies. This data has also provided new transparency into state eligibility and enrollment processes that had previously been lacking.
CMS initially indicated it would report unwinding data only through June 2024 (the official end of the unwinding period). However, many states received CMS approval to extend timelines to complete their unwinding-related renewals. Subsequently, a May 30, 2024, State Health Official (SHO) letter announced that starting July 1, 2024, CMS will expect all states to continue to submit certain metrics contained in the Unwinding Data Report on an ongoing basis, now referred to as an “Eligibility Processing Report.”
These reports will include monthly data on:
- Renewals initiated.
- Renewals due.
- Successful renewals, including the number renewed on an ex parte basis and through pre-populated renewal forms.
- Coverage terminations due to both ineligibility and procedural reasons.
- Pending renewals and renewal backlogs.
- Fair hearing requests pending for more than 90 days.
In the SHO letter CMS also explicitly encourages states to continue state-level transparency processes, including public dashboards that “can support ongoing state-level efforts to ensure timely processing of applications and renewals.”
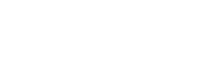
States Publicizing Medicaid Renewal Data
During the unwinding period, the State Health Access Data Assistance Center (SHADAC) tracked which states were publicly reporting unwinding data (separate from their required CMS monthly report). Over the course of the official unwinding period, from April 2023 through June 2024, 45 state Medicaid agencies (including the District of Columbia) regularly published their own renewal data (reflected in the map above), either in an interactive dashboard or a static PDF format. Two states, Mississippi and West Virginia, made copies of their monthly CMS data unwinding reports available on their state websites, but did not publish any additional state-level renewal or unwinding data. Four states, Alabama, Florida, Hawaii, and Wyoming, did not publish any state-level data.
Although some states, such as Arkansas, Idaho, Montana, and Utah, have indicated that they will no longer be updating their state unwinding dashboards, the majority of states appear to be maintaining and posting regular data updates. Other states, such as Virginia, have indicated that they plan to incorporate some of the information from their unwinding dashboard into an ongoing dashboard to track enrollment as a whole.
Medicaid Reporting Bright Spots
Given the time-lags and caveats of the CMS data, state-level dashboards and/or reports became valuable sources of timely, up-to-date information for states, policymakers, and other stakeholders, allowing them to better understand how the unwinding progressed. States that published their own data also had the ability to provide additional detail about definitions, varying timeframes, and state-specific context important for communicating the unique circumstances that they experienced during unwinding.
In addition, although CMS only required states to report data broken down by modified adjusted gross income (MAGI) and non-disability applications versus disability applications, many states were able to supplement their federal reporting with both state-specific data analysis and data broken down by eligibility group and other demographic characteristics (e.g., age, race, ethnicity, language, geography). These types of additional data breakdowns helped elucidate important trends about the disproportionate impact of the unwinding on groups that have been economically or socially marginalized.
Several states also reported how many individuals were reinstated in Medicaid after a termination, thus providing a more complete story about what happened to individuals after they were disenrolled from Medicaid.
Among state Medicaid agencies’ unwinding dashboards or reports, several stood out.
Indiana Family and Social Services Administration – Medicaid Renewals and Outcomes Dashboard
Indiana’s dashboard provided a highly visual and interactive interface for the user. Renewal outcome data was filterable by geography, race and ethnicity, gender, age, program type, and managed care entity. Renewal outcomes were displayed both as total counts and percentages.
Kentucky Cabinet for Health and Family Services – Medicaid Unwinding Demographic Reports
Kentucky was one of the earliest reporters of state-level unwinding data, publishing data snapshots beginning in April 2023. Kentucky additionally began publishing Data Demographic Reports on a monthly basis beginning in September 2023, which provided breakdowns by race, ethnicity, age, gender, and county of residence, of Medicaid renewals, pending cases, and terminated cases.
Massachusetts’ dashboard, updated on a monthly basis, provided data on member renewals and departures, filterable by age, program type, disability status, and whether the member resides in a “priority community” (i.e., one of the top 15 towns or cities where the most MassHealth members were at risk of losing coverage). Massachusetts also reported the number of terminated members who re-enrolled in Medicaid after a specific period of time.
Nevada’s dashboard displayed historical enrollment data both prior to and during the public health emergency (PHE). It also contained detailed metrics of the demographic characteristics for individuals disenrolled from Medicaid, including a comparison of the distribution of the disenrolled population versus the enrolled population. This visual display of differences between the two groups made it especially clear to see how disenrollments were affecting certain demographic groups more than others.
Oregon Department of Human Services – Medical Redeterminations Dashboard
Oregon’s dashboard displayed the number of renewals due each month as well as the number of renewals that were completed, initiated, or not started. The dashboard also presented data disaggregated by written language, gender identity, race and ethnicity, age, disability status, housing status, county, and reason for closure. Oregon also published a separate dashboard for call center data, including a daily average customer service score.
State-Based Marketplace Reporting
State-Based Marketplaces (SBMs) also played a significant role during the unwinding by coordinating with Medicaid agencies and using a number of different strategies to ensure a smooth transition for people who no longer qualified for Medicaid and were eligible for a qualified health plan (QHP) offered through the Marketplace. Given this, policymakers, advocates, and the media have also been keenly interested in unwinding data on the outcomes of transitions from Medicaid to the Marketplace.
By the end of the unwinding, 16 of the 19 states that operate an SBM had reported some data on Marketplace transition outcomes (see Table 1 below). In some states, this information was reported by the SBM itself, and in other states, Marketplace transition outcomes were included within the state’s Medicaid renewals dashboard. In 11 states, this meant ongoing reporting as part of a formal and easy to find data dashboard or data repository. In five states, Colorado, Idaho, Kentucky, Maine, and Washington, data was reported less consistently – examples include reporting as a part of SBM board meeting minutes or administrative documents, or as a part of a one-time or sporadic release of information. Three SBMs, the District of Columbia, New Mexico and Virginia, did not publicly report Marketplace transition data. Virginia, however, launched its SBM on November 1, 2023 and while the state was using the Federally-Facilitated Marketplace (FFM) at the beginning of the unwinding, CMS was responsible for the states’ reporting of transition data.
Table 1. Reporting of State-Based Marketplace Transition Data
|
State |
Marketplace Transition Data Reporting |
|
California |
|
|
Colorado |
Connect for Health Colorado Medicaid to Marketplace Bridge Update, April 2024 |
|
Connecticut |
|
|
Idaho |
|
|
Kentucky |
|
|
Maine |
|
|
Maryland |
|
|
Massachusetts |
|
|
Minnesota |
|
|
Nevada |
Monitoring Medicaid Enrollments, Disenrollments, and Renewals in Nevada |
|
New Jersey |
|
|
New York |
|
|
Pennsylvania |
|
|
Rhode Island |
|
|
Vermont |
|
|
Washington |
|
Generally, reporting of SBM data was more limited and less consistent across states than Medicaid reporting. All of the states listed in the table above reported enrollment in a QHP by people no longer enrolled in Medicaid. Only one SBM, Idaho, reported a conversion rate (i.e., Marketplace enrollment among those disenrolled from Medicaid) and about half of the SBM states reported elements allowing for this calculation (however, it is important to note that often these data points were hard to find). Six SBM states reported information about whether transitioners received premium assistance, and only two states, California and Washington, reported transitioner demographics.
Along with this data reported by SBMs, CMS also released state Marketplace enrollment transition data. These data included information on consumers who:
- Were transferred to or applied for Marketplace coverage.
- Were eligible for a QHP or Basic Health Plan (BHP) coverage (disaggregated by those eligible for financial assistance).
- Had a QHP selection or BHP enrollment.
CMS data was reported differently for FFM states that use HealthCare.gov, and for SBM states with an integrated system versus those who transfer accounts between Medicaid and the Marketplace.
While CMS data offered a somewhat parallel view of progress in all states, it was released at a lag (compared with state reported data) and comparability was complicated by data concerns and cautions regarding state comparisons, differences in how states managed changes to ex parte renewals, and potential confusion regarding the use of different denominators. Although CMS is requiring states to report ongoing Medicaid enrollment and renewal metrics beyond the unwinding period, the May 2024 SHO letter indicated that states will no longer have to report SBM transitions starting June 30, 2024, or once the state has completed all unwinding-related renewals (whichever is later).
SBM Reporting Bright Spots
While most SBM states offered transparency regarding unwinding transitions by releasing outcomes data beyond required CMS reporting, variation in how data were reported, their specific definitions, reporting timelines, and disaggregation made it very difficult to compare similar measures across states.
That said, like the Medicaid unwinding dashboards, individual SBM reporting allowed states to present the most current data available in the context of their broader unwinding efforts – controlling the narrative and storyline. In other words, states could report more quickly, and they could present Marketplace and Medicaid data together offering a holistic view of the impact of the unwinding. States could also publish disaggregated data, beyond the requirements, such as transitioner race/ethnicity and geography. States were also able to provide more detail on the metrics being released, providing clear data labels and definitions, methodologies and documenting data revisions. Among the SBM states reporting robust Marketplace transition data, several stood out.
Covered California Medi-Cal Transitioner Profile
California provided detailed data on Californians who transitioned from Medi-Cal to Covered California (the state’s official health insurance Marketplace) in the form of an Excel file. The Excel file has multiple tabs and contains counts, percentages, and detailed methodological and definitional information. It starts with a tab containing summary information on transitions by month (called “key performance indicators”). The tabs that follow contain detailed demographic information for: individuals who lost Medi-Cal and who were eligible for Covered California; those who lost Medi-Cal, were eligible for Covered California, and received an automatic plan selection; and those who effectuated QHP coverage. Demographic data available for those categories includes:
- Age
- Gender (including transgender identification)
- Income
- Race and ethnicity (in combination and separately)
- Written language
- Service channel used (i.e., Certified Insurance Agent, Certified Enrollment Counselor)
- Geography (i.e., region, county)
- Financial assistance
Pennsylvania Medicaid Continuous Coverage Unwinding Data Tracker
Pennsylvania had one of the earliest unwinding dashboards featuring Marketplace renewal outcome metrics. The dashboard presented side-by-side renewal outcome metrics for Medicaid and the Marketplace, providing a holistic view of coverage transitions across the state. In addition, the state provided information on the outcomes of transitions to Pennie (the state’s official health insurance Marketplace) by county and ZIP code.
Washington Keeping People Covered During the Medicaid Unwind: Data Snapshot Reports
Washington released robust data snapshots in October 2023 and January 2024 (each available as a PDF). These reports started with summary information (called “data top lines”), a personalized coverage transition example illustrating an individual’s cost under a QHP, and detailed information on coverage transitions such as the geographic distribution, carrier transitions, receipt of financial assistance, and demographics of transitioners (i.e., age, sex, race, and ethnicity). Washington provided both counts and percentages for most data points and provides a detailed appendix with information on data sources and definitions.
Conclusion
Timely, accessible, state-level data on Medicaid renewal outcomes will continue to be important for understanding the impact of various policies on Medicaid enrollees, even after the unwinding period ends. Given the ongoing reporting requirement from CMS, and states’ success setting up these new public reporting capabilities, there is hope that states will continue to make detailed disenrollment, renewal, call center, and Marketplace transition data publicly available on an ongoing basis.
Blog & News

Disability Health Care Data and Information: Resources from SHADAC
January 09, 2025:- Unfair treatment in health care settings, at work, or when applying for public benefits
- Adults with disabilities are more likely to live in poverty compared to adults with no disability
- People with a disability often have increased medical expenses, with a study from the National Disability Institute estimating that a U.S. household containing an adult with a disability must spend an estimated 28% more income to obtain the same standard of living as a household with no disability
- Those with disabilities have twice the risk of developing chronic health conditions like depression, diabetes, asthma, and poor oral health
Federal Survey Sample Size Analysis: Disability, Language, and Sexual Orientation and Gender Identity
- People who indicated sexual orientation or gender identity (SOGI)
- People with language access needs, and
- People with disabilities
Collection of Self-Reported Disability Data in Medicaid Applications: A Fifty-State Review of the Current Landscape (SHVS Brief)

State Health Compare Disability Breakdowns
Housing Affordability Matters: Unaffordable Rents Infographics Updated with 2022 Data

Minnesota Community and Uninsured Profile
Stay Informed on Disability Health Data Resources and Information
Blog & News
LGBT Health Equity: Sexual Orientation and Gender Identity Data Resources and Information from SHADAC
October 28, 2024:- Less likely to have health insurance coverage
- Less likely to have a regular health care provider
- More likely to delay care
- More likely to report poor quality care and unfair treatment from providers
Sexual Orientation and Gender Identity Data: New and Updated Information on Federal Guidance and Medicaid Data Collection Practices (SHVS Brief)
State Health Compare: Explore Health Data with SOGI Data Breakdowns
- Adults Who Forgo Needed Medical Care Due to Cost
- Adult Smoking
- Adult Excessive Alcohol Consumption
- Adult E-Cigarette Use
- Chronic Disease Prevalence
- Adult Unhealthy Days
- Activities Limited Due to Health Difficulty
- Adults with No Personal Doctor
- Adult Cancer Screenings
- Adult Flu Vaccinations
Gender Based Discrimination in Health Care by Gender Identity in Minnesota

- Over half (57.1%) of trans and non-binary people reported forgone care—more than double the overall average of 26.2%
- Nearly one-third of trans and non-binary adults had low confidence in getting necessary health care—compared to the overall average of 11.8%
Examining Discrimination and Health Care Access by Sexual Orientation in Minnesota
- Both lesbian/gay and bisexual/pansexual people were more likely to report barriers to health care access
- Bisexual/pansexual people were more likely to report having low confidence in the ability to get needed health care
- Both lesbian/gay or bisexual/pansexual people had significantly higher rates of forgone care
SHADAC Response to 2023 Request for Comments on American Community Survey SOGI Questions
Stay Up to Date on the Latest in SOGI and LGBT Health Data
Blog & News
Hartman, Lacey
Lukanen, Elizabeth
Changes to Child and Adult Core Sets to Advance Equity (SHVS Cross-Post)
July 02, 2024:
The following Expert Perspective (EP) is cross-posted from State Health & Value Strategies. Authors: Elizabeth Lukanen and Lacey Hartman, SHADAC
Original posting date June 7, 2024. Find the original post here on the SHVS website.
The Child and Adult Core Sets were established to measure the quality of care for Medicaid and Children’s Health Insurance Program (CHIP) enrollees, nationally and at the state level, based on a uniform set of measures. The goal of the Core Sets is to monitor performance and improve the quality of healthcare. Starting in fiscal year (FY) 2025, states will be required to report a subset of Child and Adult Core Set measures (see Table 1) by race and ethnicity, sex, and geography.
By requiring data disaggregation for key populations of interest, policymakers, advocates and researchers will have a new tool to measure, monitor and inform policies and practices that focus on health equity.
Table 1: Core Set Measures Subject to Stratification (10 Measures in Total)
|
Child Core Set Measures (7 of 27 measures) |
|||
|
Measure Name |
National Quality Forum (NQF) # |
Measure Steward |
Data Collection Method |
|
Well-Child Visits in the First 30 Months of Life (W30-CH) |
1392 |
National Committee for Quality Assurance (NCQA) |
Administrative |
|
Child and Adolescent Well-Care Visits (WCV–CH) |
1516 |
NCQA |
Administrative |
|
Oral Evaluation, Dental Services (OEV-CH) |
2517 |
Dental Quality Alliance (DQA) (American Dental Association) |
Administrative |
|
Follow-Up After Hospitalization for Mental Illness: Ages 6 to 17 (FUH-CH) |
576 |
NCQA |
Administrative |
|
Prenatal and Postpartum Care Up to Age 20 (PPC2-CH) |
1517* |
NCQA |
Administrative or hybrid |
|
Live Births Weighing Less Than 2,500 Grams (LBW–CH) – CMS calculates on behalf of states |
1382 |
Centers for Disease Control and Prevention (CDC)/National Center for Health Statistics (NCHS) |
State vital records |
|
Low-Risk Cesarean Delivery (LRCD-CH) – |
Not applicable |
CDC/NCHS |
State vital records |
|
Adult Core Set Behavioral Health Measures (3 of 11 measures) |
|||
|
Measure Name |
NQF # |
Measure Steward |
Data Collection Method |
|
Initiation and Engagement of Substance Use Disorder Treatment (IET-AD) |
0004 |
NCQA |
Administrative or electronic health record |
|
Follow-Up After Emergency Department Visit for Substance Use: Age 18 and Older (FUA-AD) |
3488 |
NCQA |
Administrative |
|
Follow-Up After Hospitalization for Mental Illness: Ages 18 and older (FUH-AD) |
0576 |
NCQA |
Administrative |
*No longer endorsed by NQF.
States will be required to stratify these mandatory measures using the following categories:
- Race and ethnicity: Using the newly released 2024 Revisions to the Office of Management and Budget’s Statistical Policy Directive No. 15: Standards for Maintaining, Collecting, and Presenting Federal Data on Race and Ethnicity. Minimum categories include:
- American Indian or Alaska Native
- Asian
- Black or African American
- Hispanic or Latino
- Middle Eastern or North African
- Native Hawaiian or Pacific Islander
- White
- Sex: Defined as biologic sex, using the 2011 HHS Implementation Guidance on Data Collection Standards for Race, Ethnicity, Sex, Primary Language, and Disability Status. Categories include:
- Male
- Female
- Geography: Using the core-based statistical area (CBSA), which are county-based statistical areas defined by large population areas, as a minimum standard. Those categories include:
- Metropolitan statistical area (population core of 50,000 or more)
- Micropolitan statistical area (population core of 10,000 to 49,999)
- Outside Core Based statistical area
Background and Context
Every year, the Secretary of the U.S. Department of Health and Human Services is required to review and update the Child and Adult Core Sets. This review is designed to detect measurement gaps and to identify and recommend revisions to improve and strengthen the Core Sets. This review is led by a workgroup that includes input from a variety of stakeholders including states, managed care plans, healthcare providers, and quality experts. In response to the annual review process, state reporting of these measures has evolved and starting in FY 2024, reporting of the Child Core Set and the Core Set of behavioral health measures for adults enrolled in Medicaid became mandatory.
Over time, the Core Sets have been specifically recognized as a critical tool to monitor health disparities. Increasing stratification of the measures is a priority area for the Centers for Medicare & Medicaid Services (CMS) and in guidance released in 2022, CMS explicitly encouraged states to “use Core Set data to identify disparities in care and to develop targeted quality improvement efforts to advance health equity.”
During the review of the 2025 Core Set Measures, the Core Set review workgroup discussed using stratified Core Sets data to advance health equity. Workgroup members who represent state and enrollee perspectives both highlighted the importance of disaggregation for assessing member experience and monitoring equity while also acknowledging the challenges inherent to data collection and reporting. In response to this discussion, the following challenges and considerations were highlighted in the final FY 2025 recommendations report:
- Data on enrollee demographics is of variable quality, with missing and unknown data (enrollees who don’t provide data and related hesitancy).
- Administrative burden to collect this information.
- Political considerations for how the data are collected and reported (balancing state legislative agendas compared to CMS requirements).
- Technical challenges, such as having multiple conflicting sources of data.
- Misalignment of reporting stratification categories with other federal and state program requirements.
- Need to engage enrollees in the collection and use of these data.
- Need for technical assistance to states to meet the new reporting requirements.
Despite these challenges, there was consensus among the workgroup about the importance of stratification, which aligned with the new requirement that 10 measures be reported by race and ethnicity, sex, and geography. Specifically, for FY 2025 reporting, states will be required to report stratified data for the seven Child Core Set measures listed above in Table 1 (25% of the 27 measures) and three of the Adult Core Set behavioral health measures (25% of 11 behavioral health measures).
Required stratification of additional measures will increase over time and the intent is that all eligible mandatory Core Set measures will be disaggregated by FY 2028. States have the option of reporting stratified data for all measures starting in FY 2025.
People’s experience of health inequities based on race and ethnicity, sexual orientation, gender identity, geography, immigration status, and other factors, is a longstanding and pervasive problem that is deeply rooted in discrimination and structural racism. The Medicaid program, through its policy, financial, and programmatic levers, is uniquely situated to address the health inequities experienced by the program’s diverse population of enrollees. Key to these efforts is the availability of comparable state programmatic and performance data to identify and track progress.
For this reason, the move toward disaggregated Core Sets data by race and ethnicity, sex, and geography is an important step to improve the monitoring of health care access and quality for Medicaid enrollees, to further identify where disparities exist and to develop and evaluate quality improvement efforts. However, this is a small step that needs to expand to identify other groups that have been economically and socially marginalized such as those with a disability, individuals who identify as lesbian, gay, bisexual, transgender, queer, intersex, or outside the gender binary (LGBTQI+), and those with limited English proficiency.
In addition to expanding data disaggregation to include a broader range of groups, it will also be important to provide states with the necessary resources and technical assistance to analyze and report these data in an accurate and comparable way. As was also noted in comments to the workgroup, enrollee engagement in the collection and use of these data is also key for advancing health equity. Community engagement is a way to establish and build trust and to develop interventions informed by the lived experience of Medicaid enrollees.
Finally, it will be critical to provide states, providers, and community partners with the resources and tools necessary to ensure that timely action is taken to actually address, and not just report on, systemic inequities.
Want to stay informed on the latest data collection practices, survey updates, and more? Sign up for our monthly newsletter here, and find health equity resources here on the SHVS site.