 VISIT STATE HEALTH COMPARE
VISIT STATE HEALTH COMPARE
Blog & News





Issue Brief: Unwinding the Medicaid Continuous Coverage Requirement - Transitioning to Employer-Sponsored Coverage (State Health & Value Strategies Cross-Post)
January 2023:The following content is cross-posted from State Health and Value Strategies, published on January 19, 2023.
Authors: Elizabeth Lukanen and Robert Hest, SHADAC
 Medicaid and the Children’s Health Insurance Program (CHIP) have played a key role in the response to the COVID-19 pandemic, providing a vital source of health coverage for millions of people. The Families First Coronavirus Response Act (FFCRA) implemented a continuous coverage requirement in Medicaid, coupled with an increase in federal payments to states. The requirement has prevented states from disenrolling Medicaid enrollees, except in limited circumstances, allowing millions of Americans continued access to healthcare services during the pandemic.
Medicaid and the Children’s Health Insurance Program (CHIP) have played a key role in the response to the COVID-19 pandemic, providing a vital source of health coverage for millions of people. The Families First Coronavirus Response Act (FFCRA) implemented a continuous coverage requirement in Medicaid, coupled with an increase in federal payments to states. The requirement has prevented states from disenrolling Medicaid enrollees, except in limited circumstances, allowing millions of Americans continued access to healthcare services during the pandemic.
Enrollment in Medicaid and CHIP has grown sharply since February 2020, with more than 20 million enrollees added to state rosters as of September 2022. Continuous coverage can also likely be credited for the decrease in the number of people who were uninsured in 2021, down to 8.6% from a pre-pandemic level of 9.2% in 2019. This was driven by a 1.4 percentage point increase in public coverage in 2021, to 36.8% from 35.4% in 2019. These trends were mirrored across states, with 28 states experiencing significant decreases in their rates of uninsurance. Meanwhile, 36 states saw rising rates of public coverage with none seeing a decline in public coverage.
When the unwinding of the Medicaid continuous coverage requirement begins, states will restart eligibility redeterminations, and millions of Medicaid enrollees will be at risk of losing their coverage. Estimates vary, but most approximate that in the range of 15 million to 18 million people will lose Medicaid coverage, with some portion exiting because they are no longer eligible, some losing coverage due to administrative challenges despite continued eligibility, and some transitioning to another source of coverage. While much attention has been paid to how states can approach the unwinding of the continuous coverage requirement to prioritize the retention of Medicaid coverage and transitions to marketplace coverage, less attention has been paid to the role of employer-sponsored insurance.
To get a sense for the size of the group that might have employer-sponsored coverage as an option, this issue brief discusses the proportion of individuals with an offer of employer-sponsored coverage by income and state, and the proportion of those offers that are considered affordable based on premium cost. The issue brief also discusses the importance of a Medicaid disenrollment survey to monitor the coverage transitions associated with the unwinding.
A companion issue brief, Helping Consumers Navigate Medicaid, the Marketplace, and Employer Coverage, discusses how state Medicaid agencies, state-based marketplaces, labor departments, and employers can play critical roles in helping people understand and navigate their employer coverage options.
To support communications efforts during the unwinding, SHVS has also produced sample messaging for state departments of labor to share with the employer community which explains the unwinding and coverage options for employees.
Blog & News

Expert Perspective and Issue Brief: Tracking the Data on Medicaid’s Continuous Coverage Unwinding (State Health & Value Strategies Cross-Post)
January 21, 2022:The following content is cross-posted from State Health and Value Strategies published on January 21, 2022.
Authors: Emily Zylla, Elizabeth Lukanen, and Lindsey Theis, SHADAC

Medicaid and Children’s Health Insurance Plan (CHIP) programs have played a key role in the response to the COVID-19 pandemic, providing a vital source of health coverage for millions of people. However, when the Families First Coronavirus Response Act (FFCRA) Medicaid “continuous coverage” requirement is discontinued states will restart eligibility redeterminations, and millions of Medicaid enrollees will be at risk of losing their coveragei.
A lack of publicly available data on Medicaid enrollment, renewal, and disenrollment makes it difficult to understand exactly who is losing Medicaid coverage and for what reasons. Publishing timely data in an easy-to-digest, visually appealing way would help improve the transparency, accountability, and equity of the Medicaid program. It would inform key stakeholders, including state staff, policymakers, and advocates, allowing them to more fully understand the impacts of Medicaid policy changes on enrollees’ access, and give them an opportunity to modify or implement intervention strategies as needed. States already collect a significant amount of data that could inform their success in enrolling and retaining eligible individuals in Medicaid. Many advocates and researchers have been calling for increased transparency around this data in order to better understand the barriers and challenges individuals face when trying to enroll in or maintain coverage.
One effective way to monitor this dynamic issue is by creating and publishing a Medicaid enrollment and retention dashboard. A typical data dashboard is designed to organize complex data in an easy-to-digest visual format, thus allowing the audience to easily interpret key trends and patterns at a glance. A new issue brief examines the current status of Medicaid enrollment and retention data collection, summarizes potential forthcoming reporting requirements, and describes some of the best practices when developing a data dashboard to display this type of information.
The issue brief lays out a phased set of priority measures and provides a model enrollment and retention dashboard template that states can use to monitor both the short-term impacts of phasing out public health emergency (PHE) protections and continuous coverage requirements, as well as longer-term enrollment and retention trends.
State Medicaid Enrollment and Retention Dashboard – Measurement Priorities
 Priority 1 – Use currently reported data: Start with the data that are already collected and submitted to the Centers for Medicare & Medicaid Services (CMS) under the 11 Medicaid performance topics.
Priority 1 – Use currently reported data: Start with the data that are already collected and submitted to the Centers for Medicare & Medicaid Services (CMS) under the 11 Medicaid performance topics.
Priority 2 – Track reasons for disenrollment: Include measures in the proposed Build Back Better Act (BBB) legislative language that address the reasons why people are being disenrolled.
Priority 3 – Monitor coverage transitions: Add measures to address issues of transitions between programs and churn—the moving in and out of coverage—that frequently occurs in Medicaid and CHIP.
Priority 4 – Explore reasons for and consequences of disenrollment: Field disenrollment surveys that could provide quantitative and qualitative data that could be used to understand both the enrollee’s experience navigating Medicaid processes as well as the consequences of disenrollment.
Regardless of the measures highlighted, an overarching goal of any Medicaid enrollment and retention dashboard should be a focus on displaying disaggregated data. Providing data broken down by various population characteristics (e.g., age, race/ethnicity, income, gender, language, or program type) or geographic areas (urban, rural) will make it easier to understand the potentially disproportionate impact of administrative enrollment and renewal policies on communities of color, persons with lower incomes, and other populations that face disparities. Access to this type of granular data provides stakeholders an opportunity to take action in order to minimize needless loss of coverage.
Designing an easy-to-understand dashboard that is accessible to all interested stakeholders—state or county program staff, navigators or enrollment assisters, and advocates—will highlight the early warning signs of large numbers of people losing Medicaid coverage. States should start small, using data dashboard best practices and as they gain experience publicly reporting this data, consider adding additional measures over time.
i Buettgens, M. & Green, A. (September 2021). What Will Happen to Unprecedented High Medicaid Enrollment after the Public Health Emergency? [Research report]. Urban Institute. https://www.urban.org/sites/default/files/publication/104785/what-will-happen-to-unprecedented-high-medicaid-enrollment-after-the-public-health-emergency_0.pd
Blog & News
A New Brief Examines the Collection of Sexual Orientation and Gender Identity (SOGI) Data at the Federal Level and in Medicaid
October 2021:Thirteen million people identify as part of a sexual or gender minority (SGM) in the United States, with an estimated 1.17 million who have Medicaid as their primary source of health insurance coverage.[1],[2] While the COVID crisis shed a unique light on the need for more equitable health data collection across all populations, one area in which efforts are still falling short is sexual orientation and gender identity (SOGI) data – especially for those covered by Medicaid. However, change is happening, and states are leading the way.
A new State Health and Value Strategies brief, authored by SHADAC researchers, documents a few examples of SOGI data collection efforts occurring at the federal level and in Medicaid, and highlights the efforts of an Oregon community stakeholder process that identified several key areas for SOGI data improvement.
 SOGI Data at the Federal Level
SOGI Data at the Federal Level
Unfortunately, there is no current federal data standard for sexual orientation and gender identity. The data standard from the Department of Health and Human Services (HHS), released in 2011, defines the category of “sex” only as biological sex and makes no mention of gender or gender identity. Additionally, when SOGI data collection efforts have been made over the past decade, certain aspects have been more routinely measured than others. For instance, most of the research to-date has focused on how to collect sexual orientation, and very little continues to be known about the best way to collect gender identity. A review in 2016, for example, found that of the 12 federal surveys that collect various aspects of SOGI information, only half of those collect information on gender identity.
SOGI Data in Medicaid
The collection of SOGI data in Medicaid is even less common than in federal surveys. SHADAC’s review of state Medicaid applications identified only two states that provided applicants an opportunity to select something other than “male” or “female” when asked to indicate their sex/gender (these terms were used interchangeably to refer to biological sex). Connecticut’s paper application has an open-text write-in option for “gender.” Oregon asks applicants to indicate their “sex assigned at birth” as well as their “gender identity.”
Improving the Collection of SOGI Data – The Oregon Model
There are still many unresolved methodological and conceptual issues when it comes to the collection of SOGI information, and very limited research assessing the validity of SOGI data specifically collected via the Medicaid application process. But one state leading the way in this effort is Oregon.
In 2018, the Oregon Health Authority (OHA) Office of Equity and Inclusion convened a SOGI Data Collection Workgroup, composed of stakeholders who interact with the Lesbian, Gay, Bisexual, Transgender, Queer, and other (LGBTQ+) community and health systems, many of whom also identify as LGBTQ+ themselves, to develop a set of SOGI data standards. The group recommended a key set of five demographic questions and response options, some open-ended for the respondent to be able to write an answer and some with the ability to check more than one categorical box, if appropriate. Options were also given for the respondent to say that they either did not want to answer or did not know what the question was asking. The workgroup also identified that a set of additional questions were needed in order to ensure respectful communication.
Soon these standards will be put into practice. A bill requiring OHA and the Oregon Department of Human Services to expand their existing race, ethnicity, language and disability data collection standards to include SOGI was recently passed by the state legislature. The state plans to convene a rule-making advisory committee in the winter of 2022 to finalize SOGI standards using the work group’s draft standards as a starting point.
Looking Forward
There continues to be very limited research assessing the validity of SOGI data specifically collected via the Medicaid application process. Absent any type of federal standard, states looking to explore different options to address their SOGI data collection gaps may need to modify SOGI questions depending on a variety of factors including the age, cultural background, and language preferences of their target population; as well as be mindful of the evolving terminology used to identify gender identity. Oregon serves as an excellent model for how to undertake a thoughtful community stakeholder process that can inform efforts to establish new data collection on a topic that is fluid and rapidly changing, yet vitally important for the health of Medicaid populations.
[1] Conron, K.J. & Goldberg, S.K. (April 2020). LGBT people in the US not protected by state non-discrimination statutes. UCLA School of Law, The Williams Institute. https://williamsinstitute.law.ucla.edu/wp-content/uploads/LGBT-ND-Protections-Update-Apr-2020.pdf
[2] 3. Conron, K.J. & Goldberg, S.K. (January 2018). Over half a million LGBT adults face uncertainty about health insurance coverage due to HHS guidance on Medicaid requirements. UCLA School of Law, The Williams Institute. https://williamsinstitute.law.ucla.edu/wp-content/uploads/LGBT-Medicaid-Coverage-US-Jan-2018.pdf
Blog & News
Expert Perspective: States’ Reporting of COVID-19 Health Equity Data (State Health & Value Strategies Cross-Post)
September 14, 2020:The following content is cross-posted from State Health and Value Strategies. It was first published on April 22, 2020.
Authors: Emily Zylla, Lacey Hartman & Lindsey Theis - SHADAC
Throughout the coronavirus pandemic SHADAC has been tracking which states are regularly reporting data that could help shed light on the health equity issues of this crisis. Collecting disaggregated demographic data on the impact of COVID-19 is one way to advance health equity during response efforts. We have found that all states are reporting some data on the coronavirus (COVID-19) outbreak, but the type and granularity of information varies considerably across states. In this expert perspective we provide updated interactive maps that explore the current status of all 50 states and the District of Columbia’s reporting of COVID-19 case and death data breakdowns by age, gender, race, ethnicity, and health care workers; and provide an update on the status of states’ reporting of hospitalization and testing data by demographic categories. We also highlight examples of states that are undertaking new, or additional, COVID-19 related data collection, reporting, or research activities to understand health disparities across populations. Finally, we summarize new federal guidance related to COVID-19 data reporting.
Current Status of COVID-19 Health Equity Reporting
The number of states reporting disaggregated COVID-19 case and mortality data has increased significantly since the start of the pandemic. All states now report race or ethnicity data for either COVID-19 cases or mortalities, a marked improvement from back in April when just over half (27) of states were reporting COVID-19 cases by race, and only 22 states were reporting COVID-19 deaths by race. Additionally, at the beginning of the epidemic, only three states reported information about how the distribution of cases by race/ethnicity compared to the state’s underlying population distribution. To date, 38 states are reporting their data in this way, which is helpful for understanding the extent to which COVID-19 is disproportionately impacting certain populations.
At the start of the pandemic, 13 states were reporting COVID-19 cases by residence type, and only six states were reporting deaths by residence type. Today, all states report cases by residence type, and 47 states report deaths by residence type. Similarly, the number of states reporting the number of health care workers with positive COVID-19 cases has increased from 10 to 26, and the number of states reporting COVID-19 deaths by underlying conditions has increased from 4 to 17.
We expect that as states work to comply with the new federal reporting guidance (see below), the number of states reporting disaggregated case and testing data by various indicators will continue to increase. The number of states reporting disaggregated hospitalization and testing data, however, remains low, with just over half (26) of states reporting hospitalization data breakdowns and only eight states reporting some type of testing data breakdowns.
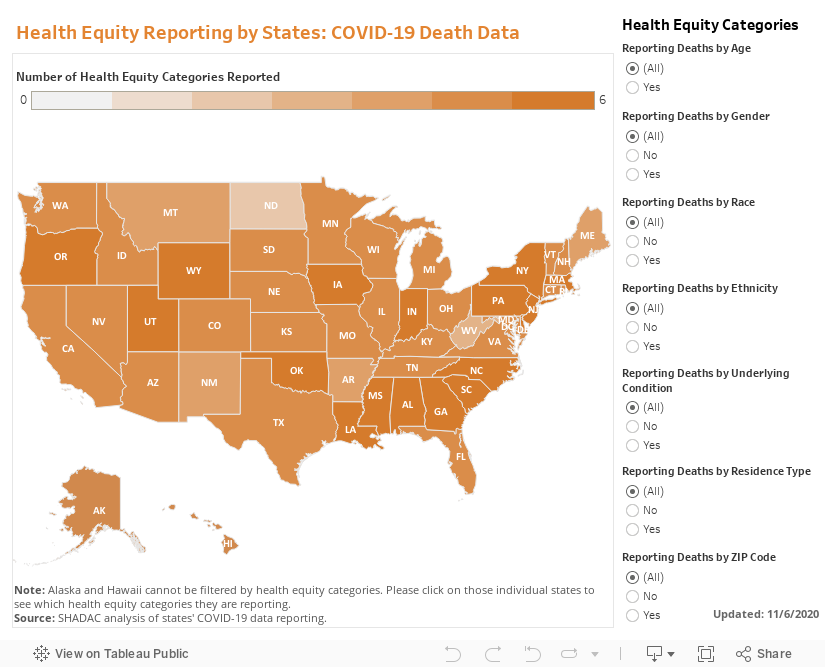
The maps below show how states are reporting disaggregated data for positive COVID-19 cases (Figure 1) and COVID-19 mortality data (Figure 2) and can be filtered to highlight which states are reporting by each health equity category. States marked by a darker shade of color are reporting more data breakdown categories than lighter-shaded states. Clicking on a state provides a link to each state’s data-reporting website along with more detailed information about which breakdowns a state is reporting.
Figure 1
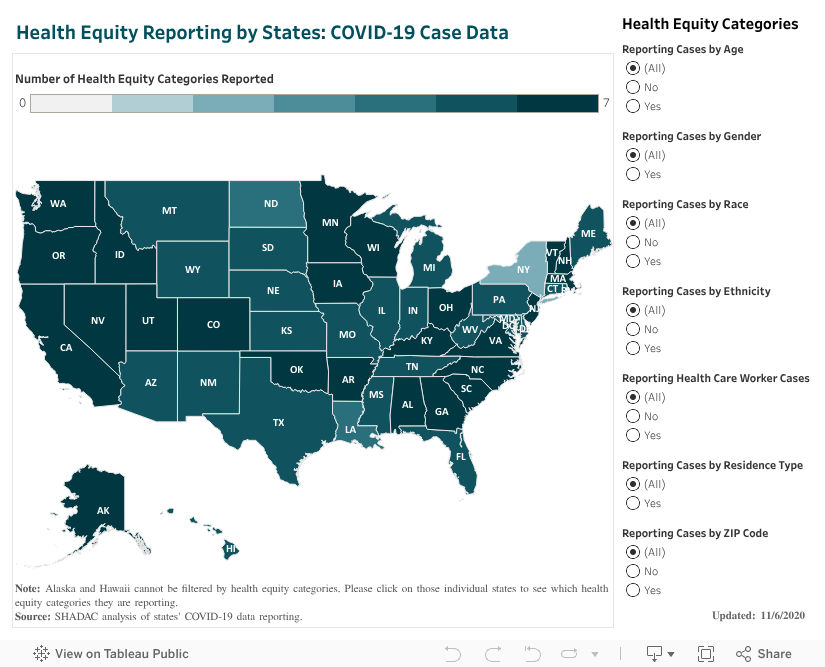
Figure 2
Hospitalizations
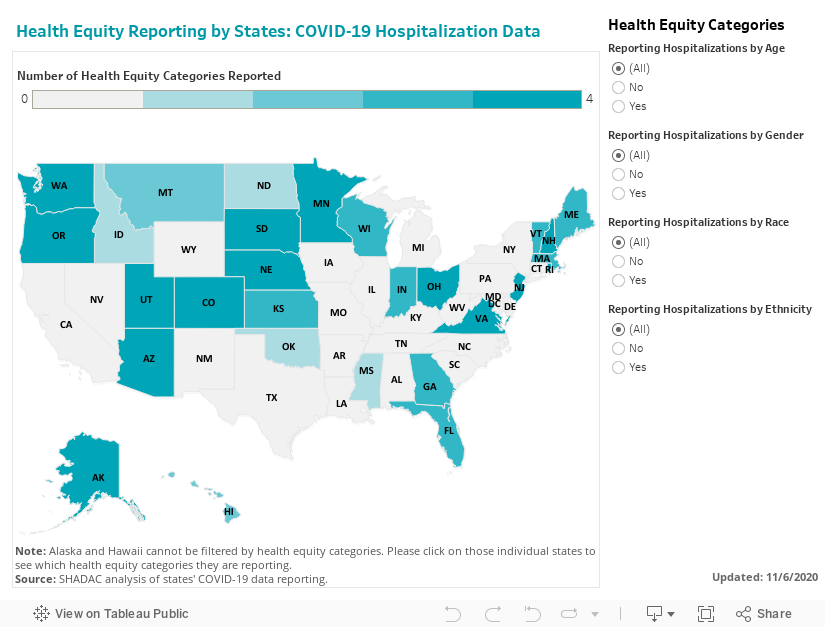
In our scan, we identified 26 states that are reporting hospitalization data for some subpopulations, but of those only 18 are reporting hospitalization data by race or ethnicity. (Figure 3.)
Figure 3
Testing
Our scan revealed eight states that are providing testing information by age and gender, and only five—Delaware, Illinois, Indiana, Kansas, and Nevada are also disaggregating testing data by race and ethnicity.
New COVID-19 Related Health Equity Data Activity
In addition to the newly required demographic data required above, several states are exploring, or beginning to report, additional data. For example:
· On September 8th, California became the first state in the nation to require the collection of sexual orientation and gender identity data for all COVID-19 patients.
· Pennsylvania announced it will work with a new data collection platform to collect sexual orientation and gender identity data.
· Minnesota is reporting language needs for positive cases interviewed and language by county of residence
· Massachusetts signed into law an act addressing COVID-19 data collection, requiring the Department of Public Health to compile, collect, and report several demographic factors, including whether an individual hospitalized speaks English as a second language.
A number of states have also formed health equity task forces, several of which are charged with looking at what additional data could be collected and reported. For example:
Colorado: A COVID-19 Health Equity Response Team, headed by the Office of Health Equity, was formed to look at inequities and ways to prevent gaps from widening during the pandemic. One of the Response Team’s tasks is to ensure racial and ethnicity COVID-19 data are accessible, transparent and used in decision-making.
Indiana: A legislative task force, led by the Indiana Black Legislative Caucus and in collaboration with the Interagency State Council on Black and Minority Health, the Indiana State Department of Health Office of Minority Health, and the Indiana Minority Health Coalition, was charged with studying racial disparities in health care and health care outcomes as it relates to COVID-19. The Task Force recommended the collection, stratification, analysis and reporting of race, ethnicity and preferred language data; and recommended action plans and annual reports of race, ethnicity, and preferred language outcomes.
Louisiana: A COVID-19 Health Equity Task Force examined how health inequities are affecting communities that are most impacted by the coronavirus. The Task Force’s Subcommittee on COVID-19 Data and Analysis made several recommendations in its report, including: establishing standardized protocols to ensure that information is consistently collected across the multiple testing sites, especially those pertaining to racial and ethnic identity; ensuring data collection occurs in collaboration with trusted organizations, e.g. tribal organizations and faith-based organizations or nonprofits within the Asian community; creating a data warehouse where harmonized data can be easily extracted for analysis; and allocating resources allocated to the Louisiana Department of Health to accomplish these goals.
Michigan: The Michigan Coronavirus Task Force on Racial Disparities serves as an advisory board within the state's Department of Health and Human Services. Among several charges, the Task Force will: study racial disparities of COVID-19 in Michigan and recommend action to overcome the disparities; recommend actions to increase transparency in reporting data regarding the racial and ethnic impact of COVID-19 and remove barriers to accessing physical and mental health services; and ensure stakeholders are informed, educated, and empowered with information on the racial disparities of COVID-19.
New Hampshire: The Governor’s COVID-19 Equity Response Team was charged with developing a recommended strategy to address the disproportionate impacts of the COVID-19 pandemic. Initial recommendations included: Adopting and following best practices (outlined in the report) for equitable data collection, analysis, dissemination, and utilization; dedicating staff with specific expertise in equitable data best-practice methodologies; and developing internal protocols that require the use of a vetted and approved Equity Review Tool analysis for all programmatic and policy work.
Ohio: The Minority Health Strike Force was charged with addressing the disproportionate impact of COVID-19 on minority populations in the state. The strike force was comprised of four subcommittees: data and research; education and outreach; health care; and resources. The groups’ Blueprint report included data-specific recommendations to improve data collection and reporting, have state agencies develop dashboards to monitor inequities and disparities, and consider the need for sufficient samples to identify disparities in groups with small population sizes. The Governor’s subsequent Executive Response included a commitment to: collect state-level health care quality information stratified by race, ethnicity, and language data; identify the contributing and confounding factor affecting the health disparities; identify and targeting the resources where interventions may be best applied; adopt of standards by state agencies to achieve a normalized set of data that uses the same categorization scheme; and establish evaluation criteria of impacts to inform policy.
Pennsylvania: The Pennsylvania COVID-19 Response Task Force on Health Disparity is charged with identifying obstacles that cause disparity for marginalized populations. The group collaborated with community members, stakeholders, and legislators to send recommendations to the Governor for addressing issues related to a higher incidence of COVID-19 among minorities. The group recommended instituting a statewide standard around racial/ethnic data collection that mirrors the standards in the Affordable Care Act, and disaggregating Asian health data.
Tennessee: The Tennessee Department of Health, Office of Minority Health, launched a statewide Health Disparities Task Force to: examine existing data, monitor trends, and hear from those living, working and serving Tennessee communities to generate responsive solutions and policies to reduce health disparities.
Vermont: A Racial Equity Task Force will undertake projects designed to promote racial, ethnic and cultural equity, including evaluating structures of support for racially diverse populations, including a focus on the racial disparities in health outcomes highlighted by COVID-19. It will submit recommendations to the Governor on the COVID-19 project by August 15.
CARES Act Reporting Requirements
In March 2020 Congress passed, and the President signed, the Coronavirus Aid, Relief, and Economic Security (CARES) Act. The statute required “every laboratory that performs or analyzes a test that is intended to detect SARSCoV-2 or to diagnose a possible case of COVID-19” to report the results from each such test to the Secretary of the Department of Health and Human Services (HHS), and authorized HHS to prescribe the form and manner of such reporting. On June 4, HHS released new guidance outlining the data elements required for reporting, which included, among other elements:
· Patient age
· Patient race
· Patient ethnicity
· Patient sex
· Patient residence zip code
· Patient residence county
· If the patient is employed in health care
· Is the patient a resident in a congregate care setting (including nursing homes, residential care for people with intellectual
and developmental disabilities, psychiatric treatment facilities, group homes, board and care homes, homeless shelter,
foster care or other)
· If the patient is hospitalized
· If the patient is pregnant
The guidance also indicates that additional data elements may be requested by state, local, or federal health departments at any time. If required data elements are not available, providers, laboratories and public health departments are encouraged to leverage resources like state, regional, or national Health Information Exchanges or Networks to obtain missing, required information. Reporting of these data elements must begin no later than August 1, 2020. While this guidance applies to all laboratories, it does not require states or local public health departments to report COVID-19 mortality data by any specific demographic breakdowns.
Blog & News
Expert Perspective: State COVID-19 Data Dashboards (State Health & Value Strategies Cross-Post)
April 10, 2020:The following content is cross-posted from State Health and Value Strategies. It was first published on April 9, 2020.
Authors: Emily Zylla and Lacey Hartman, SHADAC
Accurate, timely data is a key tool in states’ efforts to understand and respond to the impact of the coronavirus (COVID-19) outbreak at the local level. There have also been increasing calls to further break down COVID-19 data into subcategories (such as by gender, age, and race and ethnicity) in order to track the impact of the disease on specific populations. As of April 6, all 50 states and DC are publicly reporting some type of data related to COVID-19, such as the number of positive tests and/or the number of deaths. Furthermore, some states have recently begun to utilize innovative dashboards in order to visualize and track reported cases of coronavirus disease as well as monitor additional related key indicators. These dashboards are designed to organize complex data in an easy-to-digest visual format, allowing the audience to easily interpret key trends and patterns at a glance (e.g., see SHADAC’s COVID-19 dashboard template, which is currently under development using mock data).
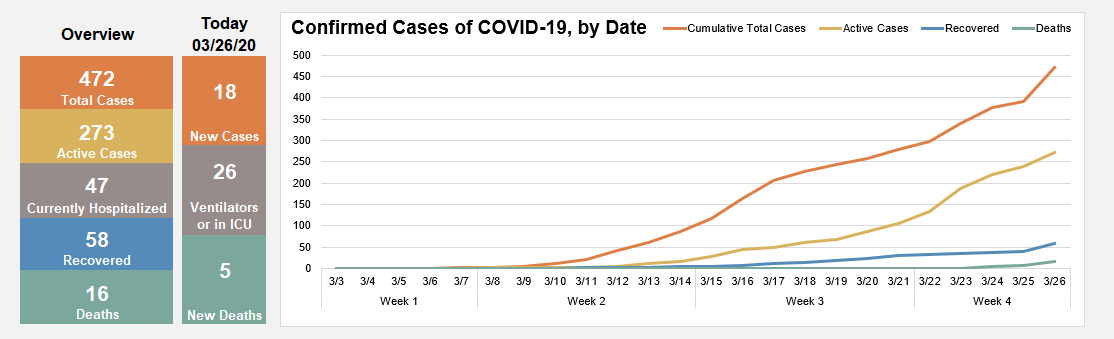
Source: SHADAC COVID-19 dashboard template under development using mock data.
This expert perspective reviews the key indicators currently being tracked by states via their COVID-19 dashboards and also provides an overview of “best practices” states can consider when developing or modifying these same COVID-19 dashboards.
| States that currently publish COVID-19 dashboards include: |
|
| Alabama | Montana |
| Alaska | Nebraska |
| Arizona | Nevada |
| Arkansas | New Jersey |
| California | North Carolina |
| Colorado | North Dakota |
| Delaware | Ohio |
| Florida | Oregon |
| Idaho | South Carolina |
| Indiana | Texas |
| Iowa | Utah |
| Kansas | Virginia |
| Louisiana | Washington |
| Maryland | West Virginia |
| Minnesota | Wyoming |
| Missouri | |
Current Status of COVID-19 Dashboards
As of April 6, we identified 31 states with public-facing COVID-19 data dashboards (i.e., the information is displayed with charts and other graphics, not just in tabular form), and we anticipate that more states will publish COVID-19 dashboards in the coming days.
States are reporting a wide number (ranging from 4 to 13) and type of indicators in their dashboards, most of which are updated at least daily.
Many states are also starting to show trends in these data points over time. The most common indicators reported on a state dashboard include:
- Number of total cases
- Number of total deaths
- Number of cases by county
- Map of cases by county
- Number of tests completed
- Number of cases by age group
- Number of cases by gender
- Number of deaths by county
- Number of hospitalizations
Other key indicators that some states are reporting that may be of interest include:
- Total number of recovered cases (i.e., cases that are no longer required to isolate)
- Number of hospitalizations that require ventilation
- Number of deaths by age/gender/race/ethnicity
- Case rate per 100,000 people by county
- Number of cases by race/ethnicity
- Number of cases by congregate living setting (e.g., long-term care, assisted living, dorms, jails, correctional settings, etc.)
- Number of tests completed by laboratory type (e.g., public vs. commercial labs)
- Number of tests completed by race/ethnicity
- Number of calls to a state’s COVID-19 hotline or number of hits on a COVID-19 website
It is important to note that states may be defining indicators that appear initially similar in different ways. For example, some states report “hospitalizations” as the total number of cases who have ever been hospitalized, while other states report “hospitalizations” as the current number of hospitalizations on a certain day. As a result, users should be cautious about making comparisons across states. In most cases, states have not identified the sources of their dashboard data beyond indicating that data is maintained by the respective state’s health department (or equivalent) and that it comes from a variety of sources such as state and local public health surveillance data, lab data (including public health, hospital, and commercial labs), and hospital reporting systems, among others. While the quality of the data being reported is difficult to assess currently (and is therefore reported as provisional), many states have acknowledged that data on confirmed cases represent an undercount due to a lack of widespread testing. Similarly, states have suggested that data on the number of deaths from COVID-19 may also change as post-mortem testing expands and guidance on how to record COVID-19 deaths is established. As mentioned below, we encourage states to include information on data quality, such as levels of missing data, where possible.
COVID-19 Dashboard Best Practices
Audience: Before designing a dashboard, make sure to clearly identify who is the intended audience. Different levels of detail, explanation, or source information may be necessary depending on whether the intended audience is state agency leadership, political leadership, or the general public. It is also important to think about what medium you will be using to reach the audience. Will the dashboard only be published on a website? Will it be available on a mobile device? Or, might you want to print it as a handout or post it on social media?
Organization and layout: Prioritize key measures. Because timeliness of these data is so important, the dashboard needs to have enough data points to convey key information, but limited enough to update quickly. It is helpful to have a landing page that makes all indicators visible to users with limited scrolling, but also provides users with the ability to “drill down” to more detail—comparisons, methodology, etc. If it is not possible to show all indicators, there should be an obvious and intuitive option for the user to “hover” over a list and get an “at a glance” view of the available content. The following example shows Florida’s COVID-19 Dashboard landing page, which implements many of these best practices.
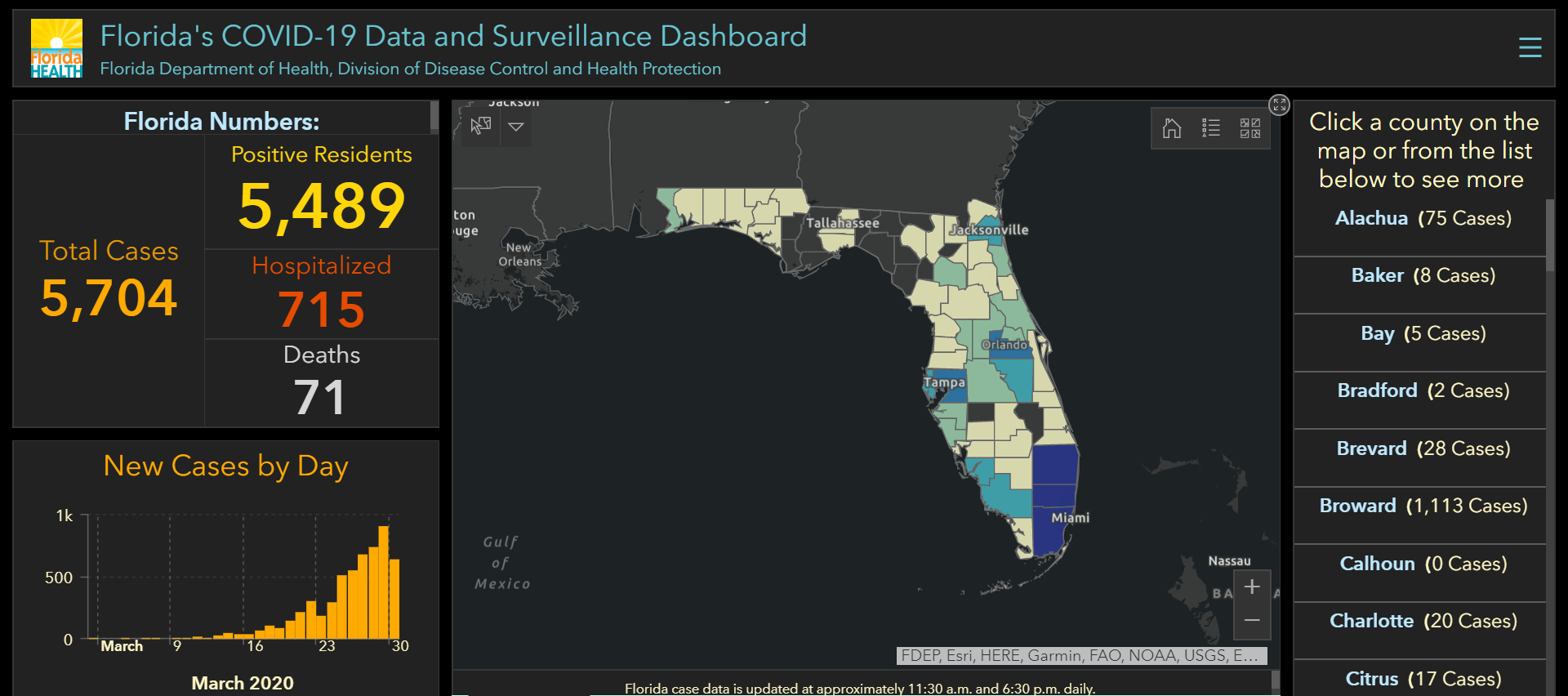
Source: Florida COVID-19 Data and Surveillance Dashboard. Accessed March 30, 2020.
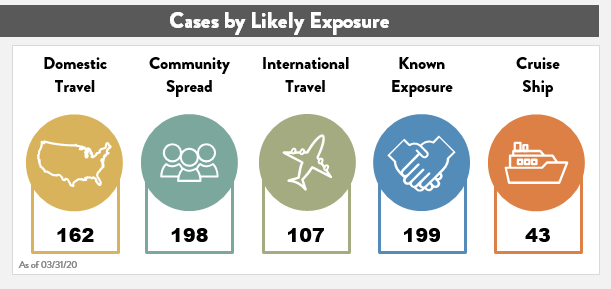
Think about any potential layout in terms of a story. It is helpful to group indicators into high-level categories with headings (e.g., overview, demographics, hospitalizations, etc.). This provides additional context for interpreting the data without the need for lengthy text descriptions. In addition, many dashboards are modular in nature so that visual elements can be replaced as information relevancy changes over time (e.g., information on likely source of exposure may become less relevant over time, while information on health care workforce exposure may become more relevant).
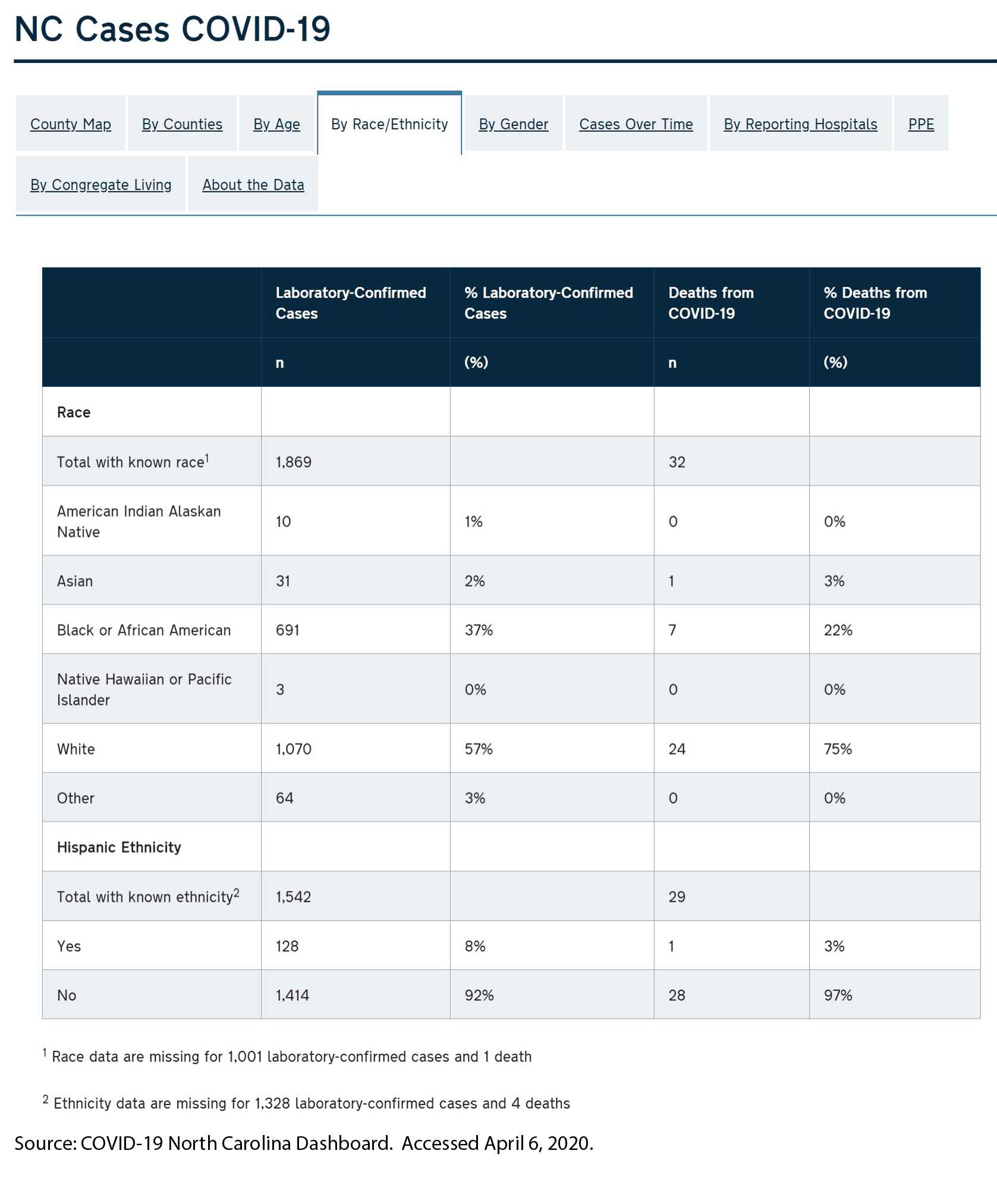
Health equity: In order to understand the potentially disproportionate impact COVID-19 may have on communities of color, low-income, and other populations that face health disparities, it will be important for states to track both COVID-19 related cases and health outcome data disaggregated for key subpopulations, such as gender, race and ethnicity, geography (e.g., urban vs. rural), and insurance status. Several states are reporting data by race/ethnicity, which is critical as early reports suggest that the crisis is disproportionately impacting communities of color. For states that do report data on race, we recommend including detail about the scope of the missing data (and the reason, if possible) to help users interpret the findings. In the example below, North Carolina’s dashboard reports confirmed cases and deaths broken down by race and ethnicity. North Carolina also clearly states the data’s limitations—i.e., the number of cases for which race and ethnicity data are missing.
Another breakdown important for monitoring equity is geography. Nearly all states are reporting data at the county level. It may also be helpful for states to present information that compares metrics in urban versus rural areas, as the unique challenges of the virus (e.g., overcrowding in densely populated areas vs. more limited hospital resources in rural areas) differ significantly by these factors. There are several approaches to defining urban versus rural areas and each have advantages and disadvantages, but given that states are already collecting COVID-19 information at the county level, it may be most straightforward to disaggregate information using the Census definition that classifies counties as “completely rural”, “mostly rural”, and “mostly urban”.
In addition to providing data by race and geography, it would be ideal if states could provide additional subpopulation breakdowns such as primary language, socioeconomic status (e.g., education, income, occupation), and disability status, if the data is available. Due to the rapid emergency response required to address the COVID-19 outbreak, we realize states may not initially have the time or bandwidth to produce a broad range of subpopulation analysis or to conduct additional analyses of their demographic data, such as looking at the intersectionality of data (e.g., by race and gender). However, those types of analyses will be increasingly important as states seek to understand disparities in COVID-19 treatment access, morbidity, and mortality.
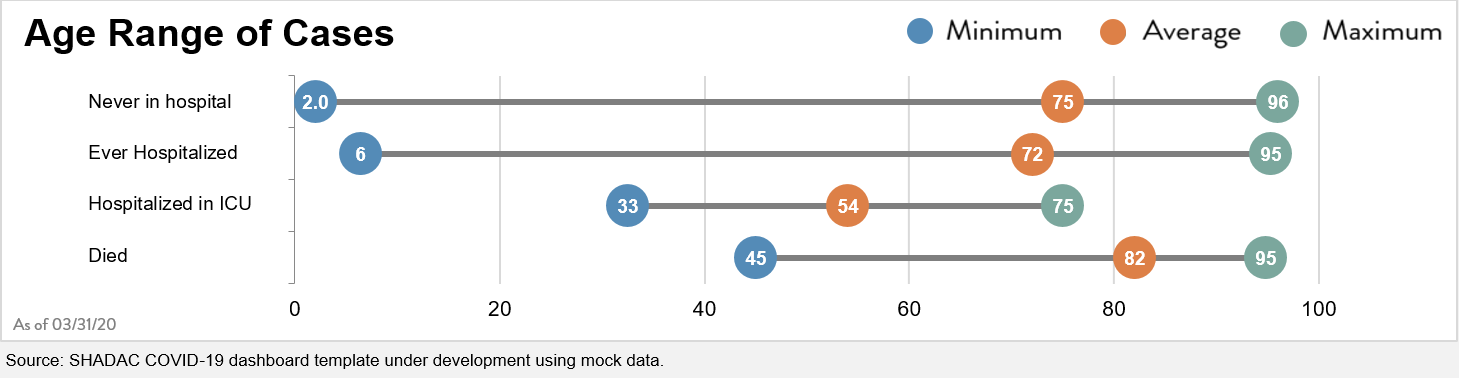
Date and time-stamps: Because these indicators are subject to change so rapidly, it will be important to date and time-stamp any dashboard updates. In addition to date-stamping the entire dashboard, also consider adding the date (and source information) to any graphic that could potentially be used as a stand-alone item in another report or on social media. For example, the graphic below represents the age distribution of a state’s COVID-19 cases and is labeled “As of 3/31/2020” so that it’s clear what time period this represents, even when the image is viewed separately from the overall dashboard.
| Data labels, definitions, and sources: Provide clear data labels and documentation. Although you should avoid “cluttering” a dashboard with extensive text, it is also important to provide the audience with information about data definitions and sources. Below is an example from North Dakota’s data dashboard showing how they included definitions for each of their six key indicators below their visualization. If space is limited, it is fine to provide hyperlinks to more detailed information on these factors. However, the links should be tested regularly to ensure they are still “live” and taking users to the correct information. 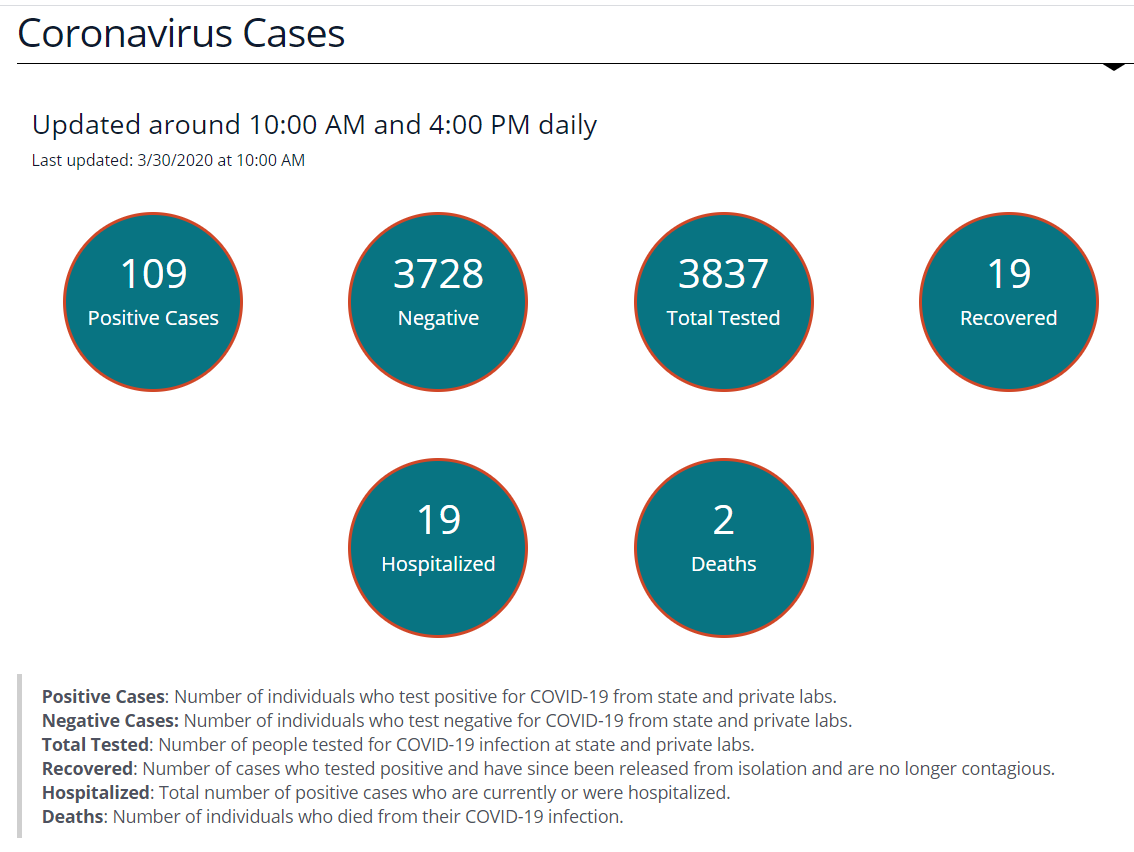 Source: North Dakota COVID-19 Dashboard. Accessed March 30, 2020. Source: North Dakota COVID-19 Dashboard. Accessed March 30, 2020. |
Time-series data: Visually displaying time-series data is an effective way to track changes. In order to improve readability, try to ensure that all time-trended data on the dashboard starts with the same date and covers the same time period, if possible. For example, although deaths and hospitalizations began ramping up at different times, these two time-trended graphs on Ohio’s dashboard start on the same date and cover the same time period. States may also choose to have a dual-axis marking both the date and the week (as shown in the first figure at the top of the page). This helps users understand the broader context of the trends being displayed. Source: State of Ohio COVD-19 Dashboard. Accessed March 30, 2020. |
 Visualizations: Choose visualizations that are clean and compliant with a range of browsers. Simple visualizations can also help users interpret more complex data “at a glance.” For example, many dashboards use up or down arrows to indicate whether most recent data show improvements or declines. Make sure visualizations require limited manual data manipulation. For example, the visual to the right was created so that it links to a back-end Excel spreadsheet, which is easily refreshed.
Visualizations: Choose visualizations that are clean and compliant with a range of browsers. Simple visualizations can also help users interpret more complex data “at a glance.” For example, many dashboards use up or down arrows to indicate whether most recent data show improvements or declines. Make sure visualizations require limited manual data manipulation. For example, the visual to the right was created so that it links to a back-end Excel spreadsheet, which is easily refreshed.
Documentation to support data updates: After constructing your customized dashboard, create an “instruction sheet” outlining all of the steps necessary to update the data on an ongoing basis, including:
- Which specific cells or inputs need daily updates
- What data sources are being used and where the data is located
- How and where to document what data was pulled and when
This detailed “instruction sheet” is especially important in the event that the individual who normally updates the data is absent or leaves—that way someone else can easily complete the update.
Support for the development of this expert perspective was provided by the Robert Wood Johnson Foundation. The views expressed here do not necessarily reflect the views of the Foundation.
Pages
- « first
- ‹ previous
- 1
- 2
- 3
- 4

