Blog & News





Household Pulse Survey (HPS) Insurance Coverage Trend Analysis: How Does It Compare?
January 10, 2024:Introduction
The U.S. Census Bureau’s Household Pulse Survey (HPS) is an online survey that provides up-to-date monthly data on emergent issues and the social and economic wellbeing of U.S. adults. As one of the only sources of publicly available rapid response data, the HPS is a critical tool for monitoring how policies such as the “unwinding” of the Medicaid continuous coverage requirement are affecting the landscape of health insurance coverage in near real time, hopefully providing actionable information for those making and implementing policy.
However, data validation of the Household Pulse Survey is crucial, especially given its short track record and novel methods. Even while offering near-real-time data, the HPS also faces several other challenges, including a notably low response rate (6.8% as of September 2023); underrepresentation of harder-to-reach demographic groups, such as adults with lower levels of education and young adults; a lack of editing and imputation for most variables; and likely some degree of nonresponse bias.
As researchers at the State Health Access Data Assistance Center (SHADAC) utilize the subannual HPS data to monitor changes in insurance coverage, we wanted to compare the HPS’ ability to detect insurance coverage changes over time against other more established surveys that also provide subannual estimates.
To this end, we compared subannual estimates of Medicaid/CHIP coverage, private coverage, and uninsurance among U.S. civilian noninstitutionalized nonelderly adults (age 18–64) in the HPS to similar estimates in the National Health Interview Survey (NHIS) [quarterly estimates from 2021–2022] and the Behavioral Risk Factor Surveillance System (BRFSS) [monthly estimates from 2022]. Below you'll find our insurance trend analysis findings using survey data.
Key Findings
Our analysis reveals that HPS estimates of coverage among adults follow similar trends as found with BRFSS and NHIS estimates. However, the exact estimates tend to deviate from each other.
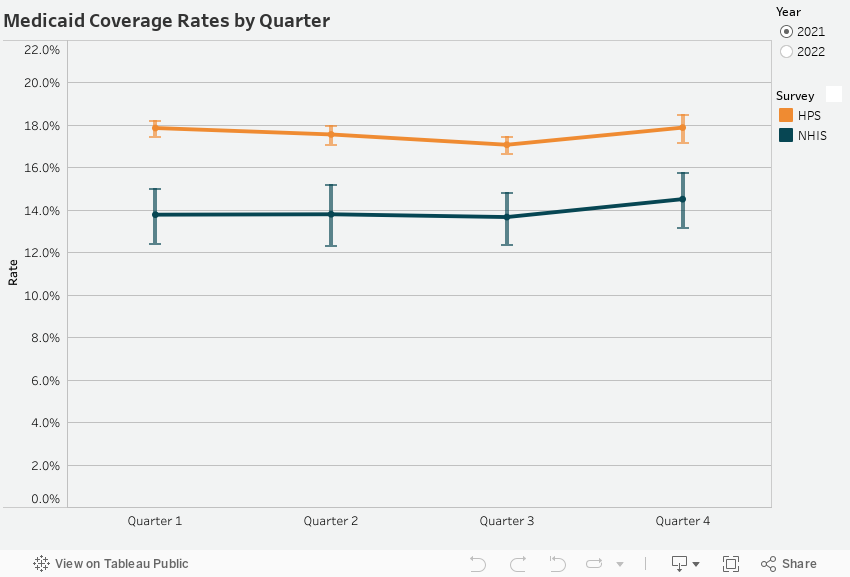
Medicaid/CHIP
HPS estimates of Medicaid coverage almost exactly follow the trend of NHIS estimates of Medicaid coverage. The HPS estimates were consistently greater than the NHIS estimates with the HPS estimating that around 18% of adults were covered by Medicaid in 2021 and around 19% in 2022. The NHIS estimates were approximately 4 percentage points lower at around 14% in 2021 and 15% in 2022.
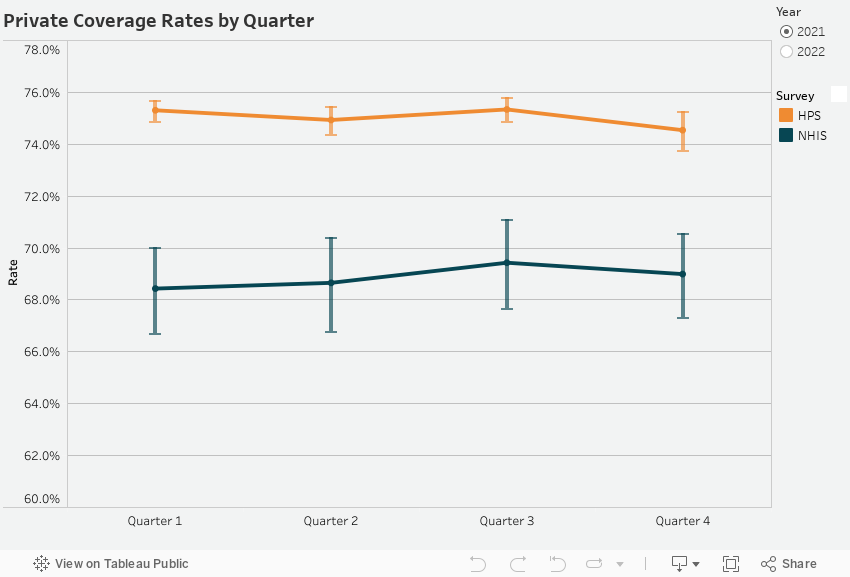
Private
Similar to estimates of Medicaid coverage among adults, the HPS estimates of private insurance coverage among adults were consistently higher than NHIS estimates, but both followed the same overall trend. HPS estimates for private insurance coverage hovered around 75% in 2021 and 2022. The gap between HPS estimates and NHIS estimates widened slightly between 2021 and 2022, increasing from an approximately 6 percentage point difference to an approximately 8 percentage point difference – NHIS estimates were around 69% in 2021 and 67% in 2022.
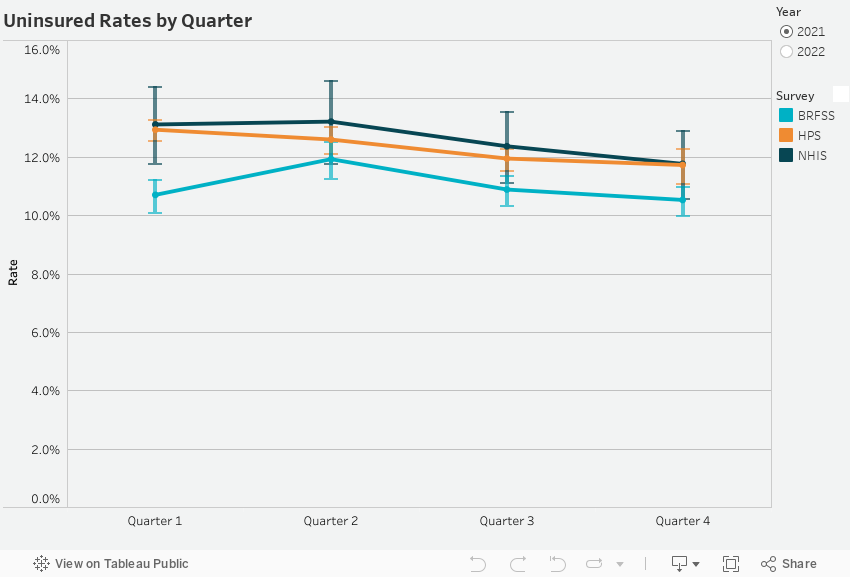
Uninsured
Similarly to both Medicaid and private coverage estimates, HPS estimates of uninsurance among adults closely mirrored the trends observed in both NHIS and BRFSS data. In a change from Medicaid and private coverage estimates, though, HPS estimates of uninsurance consistently fall between the estimates from BRFSS and NHIS, with HPS figures consistently greater than those from BRFSS but lower than NHIS’. This pattern persists through the first quarter of 2022.
Following this point, HPS estimates of uninsurance among adults decrease while BRFSS estimates increase and NHIS estimates stay more or less consistent.
Data and Methods
This analysis utilizes publicly available data from three household surveys: the Household Pulse Survey (HPS), the National Health Interview Survey (NHIS), and the Behavioral Risk Factor Surveillance System (BRFSS). All three surveys provide national representation of the civilian, noninstitutionalized population, with data collected on either a quarterly basis (NHIS) or a monthly basis (HPS and BRFSS). In order to have comparable time periods, HPS data was pooled both at the quarterly level and at the monthly level prior to analysis.
In the Household Pulse Survey, coverage was defined as having any sort of coverage (e.g. Medicaid or private) at the time of the survey. Uninsured was allocated to those that did not answer yes to being currently covered by some sort of health insurance or health coverage plan.
In the National Health Interview Survey (NHIS), Medicaid coverage among adults was defined as currently having either Medicaid coverage or CHIP coverage. Private coverage was defined as currently having any private coverage. Uninsurance was designated to those who answered they did not currently have health insurance.
The Behavioral Risk Factor Surveillance System (BRFSS) has a unique method of ascertaining health insurance coverage. As opposed to asking which health insurance coverage an individual has, BRFSS only has asks for a primary source of insurance, and individuals are only allowed to select one type of coverage. So, while BRFSS does include data on Medicaid coverage and private coverage, these estimates were not provided in this analysis as this type of instrument is not sufficiently comparable with the questions used by the HPS and NHIS to include estimates of coverage. Uninsurance among adults in BRFSS was defined as not having coverage of any type at the time of survey or being covered by Indian Health Service.
Blog & News

SHADAC Comments on Proposed 2025 American Community Survey Health Insurance Coverage Instrument Changes
January 07, 2024:The U.S. Census Bureau has released a request for comments regarding proposed revisions and changes for the 2025 American Community Survey. Based on information gained from the 2022 Content Test, proposed changes would affect a variety of topics and questions, including educational attainment, disability, household roster, and, most notably for the State Health Access Data Assistance Center (SHADAC), health insurance coverage.
See an excerpt regarding ACS health insurance coverage question changes below. You can find the full request for comments here in a notice from October 20, 2023.
| Health Insurance Coverage - Since implementation in 2008, research has found that Medicaid and other means-tested programs are underreported in the ACS and the PRCS and that direct-purchase coverage is overreported, in part due to misreporting of non-comprehensive health plans and reporting multiple coverage types for the same plan (Mach & O'Hara, 2011; Lynch et al., 2011; Boudreaux et al., 2014; O'Hara, 2010; Boudreaux et al., 2011; Boudreaux et al., 2013). Moreover, revisions to the health insurance question would help capture changes to the health insurance landscape that occurred with and since the passage of the Patient Protection and Affordable Care Act. Changes to the health insurance coverage question include a change in formatting of the question that adds an explicit response category for those who are uninsured, reordering some response options and rewording response options for direct purchase, Medicaid, employer, and veteran's health care. |
Researchers at SHADAC have reviewed the proposed changes regarding health insurance coverage data collection for the American Community Survey 2025 data year. We have crafted the following response letter discussing our opinion that the implementation of these changes be postponed in order to further investigate causes of Medicaid underreporting, and to allow for the ACS 2025 to adequately reflect effects of the Medicaid unwinding.
SHADAC’s Comments
We appreciate the opportunity to comment on Census’ proposed changes to the 2025 American Community Survey questionnaire. For more than twenty years, the State Health Access Data Assistance Center (SHADAC) has used the American Community Survey (ACS) to provide state officials and other stakeholders with data to inform health policy. Since the health insurance question was added in 2008, we have used the ACS to monitor changes in health insurance coverage.
As frequent and knowledgeable users of the survey, we have a particularly vested interest in the continued ability of the ACS to produce a high-quality measurement of health insurance coverage. With that in mind, we submit the following comments on the proposed changes to the health insurance coverage instrument. We strongly urge postponing the implementation of the proposed changes to the ACS’ health insurance coverage instrument with reasons provided below:
Medicaid Underreporting
While heartened by the commitment to improvements in the measurement of health insurance coverage, we are very concerned that the most recent content test showed significantly reduced reporting of Medicaid coverage in both versions of the test questions.
Given that this request for comment specifically mentions addressing the long-standing problem of Medicaid underreporting as a goal of the new instrument, we view this increase in Medicaid underreporting as disqualifying. In our view, Census needs to conduct further investigation to determine the cause for this demonstrated decrease in Medicaid reporting and use that information to revise the test questions to address this substantial problem.
Timing and Medicaid Unwinding Data
Though we understand that the timing for this change is driven by Census’ standard process for adding or changing survey content, we view the proposed timing of this change as inappropriate because of the ongoing, large-scale redetermination of Medicaid eligibility (“unwinding”) that began in April 2023 with the end of the pandemic-era continuous coverage requirement. This unwinding will continue into 2024.
The unwinding of the Medicaid continuous coverage requirement represents the largest nationwide coverage transition since the Affordable Care Act, and there is significant interest in monitoring the impacts. ACS data year 2025 will be the first full year of data after the completion of the unwinding.
If changes to health insurance coverage questions are implemented in 2025, we will never be able to reliably learn about the full impacts of the unwinding on health insurance coverage. Postponing revisions would allow us to better compare data and understand the impacts of the unwinding on key populations in the first full year post-unwinding completion. This is especially important for state-level populations of interest (including those relevant to furthering critical health equity goals) and for substate geographies, as the ACS is the only source of this information.
Thank you for your consideration. We know you face many important decisions and appreciate the chance to comment on this important and impactful data collection change.
See SHADAC’s comments on the newly proposed Sexual Orientation and Gender Identity (SOGI) questions on our blog here.
Blog & News

California Achieves Lowest Uninsured Rate Ever in 2022 (Cross-Post)
November 13, 2023:The following blog is cross-posted from The California Health Care Foundation.
Author: Lacey Hartman, Senior Research Fellow, SHADAC
Maintaining Gains Hinges on Transitioning People Who Lose Medi-Cal to Other Coverage in Coming Months
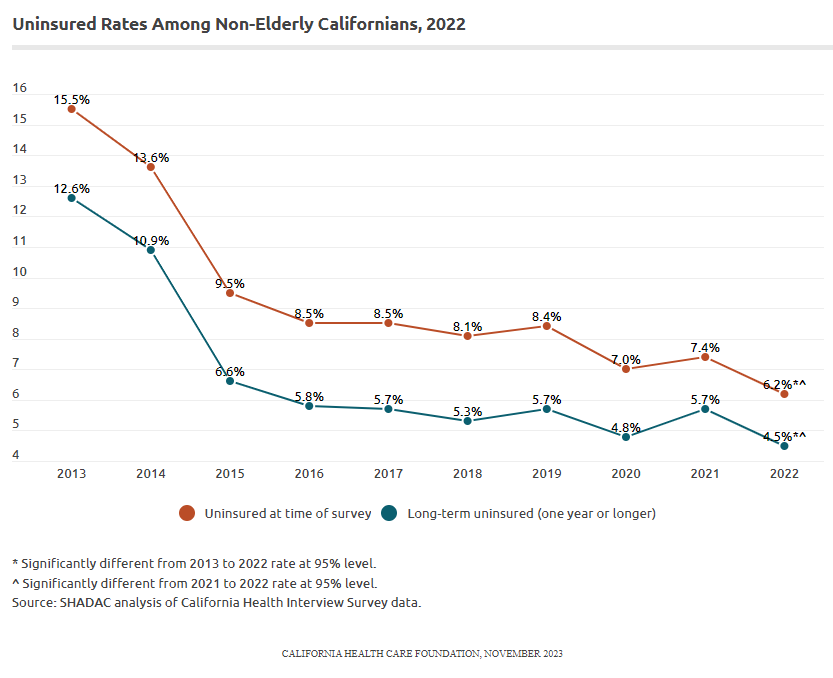
The share of Californians under age 65 (“nonelderly”) without health insurance reached a historic low in 2022. Based on the most recent California Health Interview Survey (CHIS), the percentage of nonelderly Californians without health insurance dropped to 6.2% in 2022, a statistically significant decline from 2021 (7.4%). The rate of nonelderly people without coverage for a year or more also reached a historic low in 2022. Commonly called the “long-term uninsured,” their rate dropped from 5.7% in 2021 to 4.5% in 2022, another statistically significant decline.
Disparities in Coverage by Race and Ethnicity Narrow, but Inequities Persist
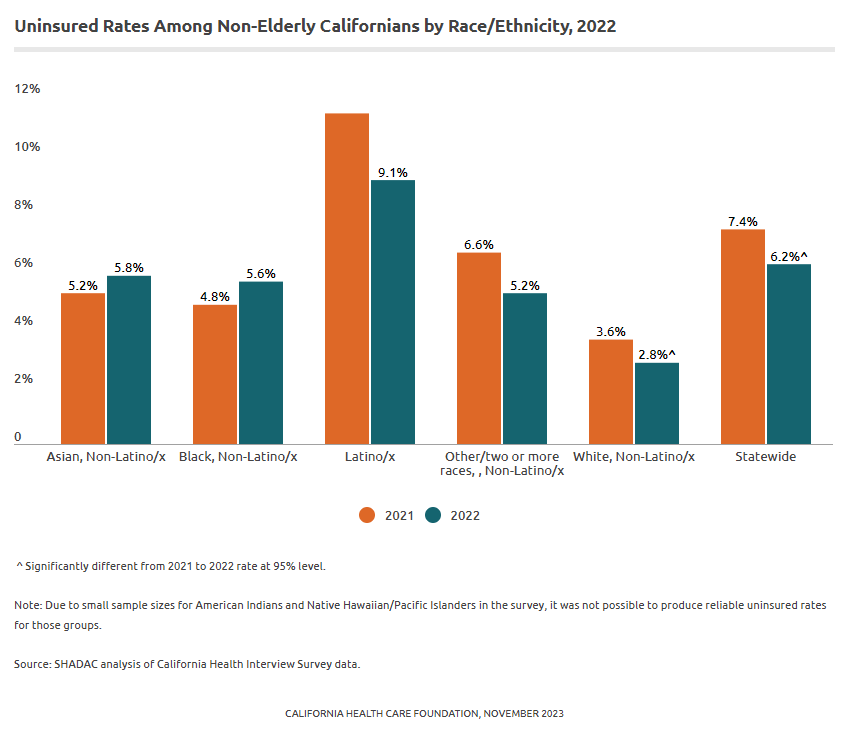
California’s Latino/x population experienced the largest improvement in coverage between 2021 and 2022; the share who reported being uninsured at the time of the survey dropped from 11.4% in 2021 to 9.1% in 2022, a change that was statistically significant. The Latino/x rate in 2022 also represents a historic low for this group.
The uninsured rate for White Californians also declined by a statistically significant but smaller amount, from 3.6% to 2.8%. There were no other statistically significant changes between 2021 and 2022 by race/ethnicity. Although there have been important gains in narrowing disparities in coverage by race and ethnicity in the state, Latino/x Californians continue to be uninsured at rates triple that of their White counterparts. Black and Asian Californians are uninsured at twice the rate of White Californians. Due to small sample sizes for American Indians and Native Hawaiian / Pacific Islanders in the survey, it was not possible to produce reliable uninsured rates for those groups.
Discussion
The fact that fewer nonelderly Californians were without coverage in 2022 than ever before is clearly good news. However, in 2023, the federal continuous coverage requirement for Medicaid came to an end. It’s estimated that as many as 2–3 million Californians may leave Medi-Cal as a result. How many Californians ultimately lose their Medi-Cal coverage and whether those leaving the program get connected to other coverage will have a huge impact on the state’s uninsured rate going forward.
These issues — as well as other challenges, such as inflation — may make holding onto California’s coverage gains difficult in the coming years. It will be vital to continue monitoring data from 2023 and future years to fully understand the impact of the pandemic — and the end of associated coverage protections, as well as other policy changes — on California’s health coverage landscape.
Blog & News
2022 ACS Tables: State and County Uninsured Rates, with Comparison Year 2021
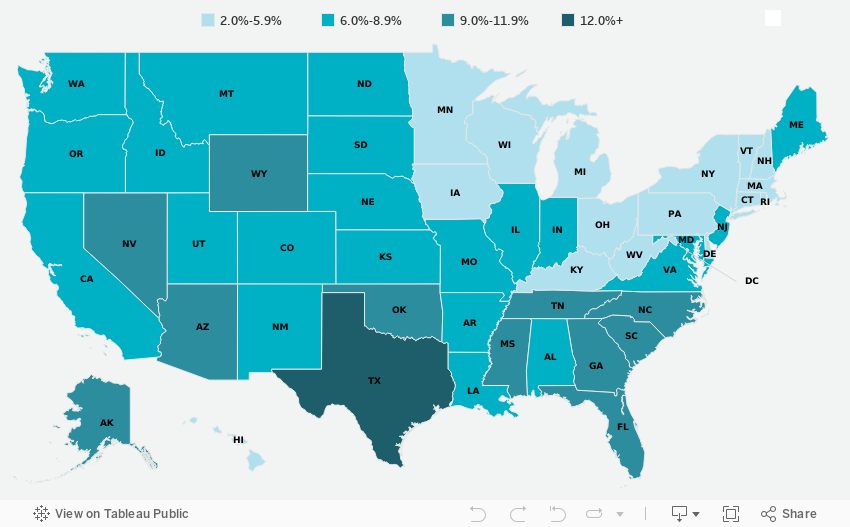
November 17, 2023:Each year, SHADAC uses data released from the American Community Survey (ACS) via the U.S. Census Bureau's data.census.gov tool to produce estimates of uninsurance at the state and county level.*
Click on a state below in the interactive map to see a PDF table of uninsured rates by state and sub-state geographies, but also by demographic characteristics (e.g., age, race/ethnicity, and poverty level) for 2022 and comparison year 2021.
Click here to view uninsurance estimates for the United States.
Click here to view uninsurance estimates for Puerto Rico and its municipios.
Note: These tables present uninsured rates, which indicate the share of the population that is uninsured. For example, a 10 percent uninsured rate for adult women indicates that 10 percent of all adult women are uninsured.
Maps & Tables of Private, Public, & Uninsured Changes from 2021 to 2022
- Private Coverage Rates by State, Change from 2021 to 2022, for All People
- Public Coverage Rates by State, Change from 2021 to 2022, for All People
- Uninsurance Rates by State, Change from 2021 to 2022, for All People
About the ACS
The ACS is a household survey that began in 2005 and produces annually updated data on a variety of population characteristics, including health insurance coverage. In total, the ACS surveys approximately three million U.S. households each year. An important feature of the ACS is that it includes a large enough sample for state‐level and sub‐state estimates.
The ACS began asking survey respondents about health insurance coverage during the 2008 calendar year. Specifically, the survey asks respondents about current coverage for each person in the respondent’s household. A person is categorized as “insured” if he or she has coverage at the point in time at which the survey is administered.
*Why Aren’t Estimates Provided for All Counties?
Due to sample size constraints, single-year ACS estimates are available at the county level only for counties with a population greater than 65,000.
How Are These Estimates Different from the Estimates that SHADAC Publishes Using Census Bureau Micro-Data Files?
Two definitions used by the Census Bureau to generate the tabulations above differ from those that SHADAC uses to generate tabulations for State Health Compare. The definitional differences are as follows:
Family
The Census Bureau defines a family as “all related people in a household.”
SHADAC defines a family using a measure called the “Health Insurance Unit” (HIU), which includes all individuals who would likely be considered a family unit in determining eligibility for either private or public coverage.
To learn more about the 2020 update of SHADAC's Health Insurance Unit (HIU) see our HIU resource page, which houses two issue briefs: The first describes the SHADAC HIU, its purpose, the most recent update, and improvements to HIU data inputs; and the second outlines the impacts of using the SHADAC HIU in analysis so that researchers can assess whether the SHADAC HIU is suitable for their research and what the potential impacts of its use might be. The page also provides a link to STATA and SAS codes to aid in the use of the HIU variable.
Family Income
The Census Bureau determines family income as a percentage of the Federal Poverty Level (FPL), which is a definition of poverty used primarily for statistical purposes. For example, FPL is used to estimate the number of Americans living in poverty each year.
SHADAC determines family income as a percentage of the U.S. Department of Health and Human Services’ Federal Poverty Guidelines (FPG), which is a measure used for administrative purposes. For example, FPG is used to determine eligibility for federal programs such as Medicaid and the Supplemental Nutrition Assistance Program (SNAP).
To learn more about the difference between FPL and FPG, read our updated blog post from April 2023.
Related ACS Materials:
- An Annual Conversation with the U.S. Census Bureau: 2022 Health Insurance Coverage Estimates from the ACS and CPS
- 2022 ACS: Declining Uninsured Rates for the U.S. and States are Supported by Private and Public Coverage Increases
- CPS ASEC: 2022 National Health Insurance Coverage Estimates Show Falling Rates of Uninsurance and Direct-Purchase Coverage (Infographic)
Publication
An Annual Conversation with the U.S. Census Bureau: 2022 Health Insurance Coverage Estimates from the ACS and CPS
On Thursday, September 28th at 1:00 PM CST, SHADAC hosted a webinar covering the release of new 2022 health insurance coverage estimates from two key, large-scale federal data sources: The American Community Survey (ACS) and the Current Population Survey (CPS).
Estimates from both surveys were presented at: the national and state levels, as well as by coverage type, and a range of other demographic categories (age, geography, poverty level, and more), during the webinar. Technical and analytic insight was provided from experts at the U.S. Census Bureau, which administers both the ACS and CPS, and SHADAC researchers joined with our special guests from the Census Bureau to answer questions from attendees after the presentation.
Attendees were able to learn about:
- New 2022 health insurance coverage estimates
- When to use which estimates from the ACS vs the CPS
- How to access the estimates via Census reports and the data.census.gov website
- How to access state-level estimates from the ACS using SHADAC tables and State Health Compare web tool
Speakers
 Kathleen T. Call, Moderator Kathleen T. Call, Moderator
Principal Investigator
SHADAC Dr. Call has been an Investigator with SHADAC since its launch in 2001. She is also a Professor in the Division of Health Policy and Management at the University of Minnesota (UMN), School of Public Health (SPH). She demonstrates her commitment to community-engaged scholarship through her leadership in the Clinical and Translational Science Institute, and the Interdisciplinary Research Leaders (IRL) program, and by co-chairing the UMN, SPH Health Equity Work Group.
|
 Katherine Keisler-Starkey, Speaker Katherine Keisler-Starkey, SpeakerEconomist in Health and Disability Statistics Branch United States Census Bureau Katherine Keisler-Starkey is an economist in the Health and Disability Statistics Branch in the U.S. Census Bureau’s Social, Economic and Housing Statistics Division. In her position, Ms. Starkey provides subject matter expertise on health topics for the Current Population Survey Annual Social and Economic Supplement (CPS ASEC) and has authored the Census Bureau’s Health Insurance Coverage in the United States report for the last four years. Her research interests focus on Applied Microeconomics, including Health Economics, Public Finance, and Labor Economics, and she is the author of several topically focused Census working papers and blogs in these areas. |
 Robert Hest, Speaker Robert Hest, SpeakerSenior Research Fellow
SHADAC Robert Hest joined SHADAC in 2017 and was recently made Senior Research Fellow. Mr. Hest provides expertise in survey data, data analysis and processing, and project management. Mr. Hest also manages SHADAC’s State Health Compare website, coordinating data processing, quality assurance, dissemination, and documentation of data.
|
 Sharon Stern, Speaker Sharon Stern, SpeakerAssistant Division Chief
United States Census Bureau Sharon Stern is the Assistant Division Chief for employment characteristics in the U.S. Census Bureau’s Social, Economic and Housing Statistics Division. In her position, Ms. Stern oversees statistics on the labor force, health insurance and disability from several Census Bureau surveys. She has authored a wide variety of Census Bureau reports and papers on topics related to poverty, disability, and health insurance.
|
Related Resources
SHADAC
- Webinar slides from SHADAC
- CPS ASEC: 2022 National Health Insurance Coverage Estimates Show Falling Rates of Uninsurance and Direct-Purchase Coverage (Infographic) (Blog)
- 2022 ACS: Declining Uninsured Rates for the U.S. and States are Supported by Private and Public Coverage Increases (Blog)
U.S. Census Bureau
- Webinar slides from Census Bureau
- Health Insurance Coverage in the United States: 2022 (Report)
- Health Insurance Coverage of U.S. Workers Increased in 2022: Health Insurance Rates for Working-Age Adults Higher by Race, Hispanic Origin, Region (Blog)
- Uninsured Rates Decreased in Over Half of U.S. States in 2022: Changes in Types of Health Insurance Coverage Contributed to Declines in Uninsured Rates From 2021 to 2022 (Blog)