*Click here to jump to the 'Systemic Racism' annotated bibliography*
The State Health Access Data Assistance Center (SHADAC) with support from the Robert Wood Johnson Foundation (RWJF) and in collaboration with partner organizations is exploring whether a new national Medicaid Equity Monitoring Tool could increase accountability for state Medicaid programs to advance health equity while also improving population health.
During the first phase of this project, a conceptual wireframe for the potential tool was created. This wireframe includes five larger sections, organized by various smaller domains, which would house the many individual concepts, measures, and factors that can influence equitable experiences and outcomes within Medicaid (see full wireframe below).
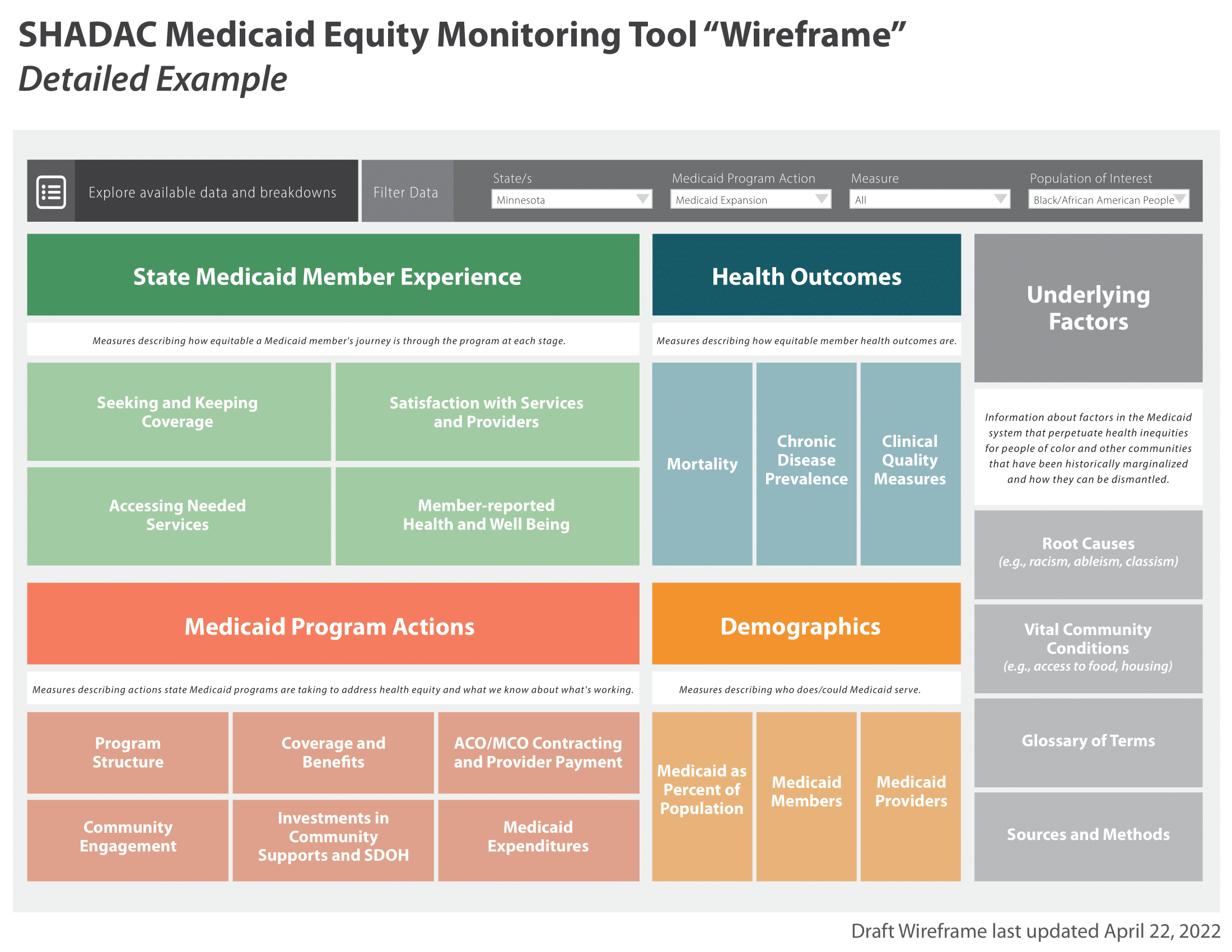
While project leaders and the Advisory Committee appointed at the beginning of the project all agree that the Medicaid program is a critical safety net, they specifically identified the importance and the need for an “Underlying Factors” section of the tool. This section aims to compile academic research and grey literature sources that explain and provide analysis for the underlying factors and root causes that may contribute to inequities in Medicaid.

These topics are complex and intersectional – the hope for the “Underlying Factors” section of a future equity monitoring tool is to break these topics down into clear, manageable, and understandable information. Researchers performed a data scan to find recent (2018 and onward) and relevant material, specifically selecting resources for inclusion that provide:
- Historical context of Medicaid inequities
- Information on how underlying factors perpetuate inequities in Medicaid
- Potential solutions for alleviating inequities within Medicaid
Once selected, researchers compiled sources in an organized annotated bibliography, providing a summary of each source and its general findings. This provides users with a curated and thorough list of resources they can use to understand the varied and interconnecting root causes of Medicaid inequities. Researchers plan to continually update this curated selection as new research and findings are identified and/or released.
Sections of the full annotated bibliography include:
- Systemic Racism
- Systemic / Structural Ableism
- Sexual Orientation, Gender Identity, and Gender Affirming Care Discrimination
- Reproductive Oppression in Health Care
- Impact on Vital Community Conditions
This page is dedicated to a single section from the full annotated bibliography:
Systemic Racism
Underlying Factors Annotated Bibliography: Systemic Racism
Have a source you'd like to submit for inclusion in our annotated bibliography? Contact us here to propose a source for inclusion.
Click on the arrows to expand / collapse each source.
Yearby, R. (2018), Racial Disparities in Health Status and Access to Healthcare: The Continuation of Inequality in the United States Due to Structural Racism. Am J Econ Sociol, 77: 1113-1152. https://doi-org.ezp1.lib.umn.edu/10.1111/ajes.12230
Author(s): Ruqaiijah Yearby, Professor of Law at Ohio State University
Article Type: Peer-reviewed journal
This article discusses the historical context and implications of Medicaid’s origins. For example, Title VI of the Civil Rights Act of 1964 was designed to support hospital-level integration but did not apply to individual-level providers, which allowed for racism to persist especially directed toward Black people. The racist conduct of providers persisted beyond Title VI, creating mistrust and deterring Black people from seeking health care even today. Yearby connects key aspects of systemic racism to health inequity, such as housing discrimination, the wealth gap, and employment discrimination. She goes on to discuss ways in which these issues are not permanent – that they can be resolved through multifaceted solutions aimed at holding institutions accountable for racial disparities in their health care, such as further diversity training for health care staff at all levels, emphasis on cultural humility over cultural competency, and, on the federal level, implementation of new anti-discrimination laws that hold institutions (such as health care systems) accountable for vast or increasing disparities among their patients.
*Another article of interest by Ruqaiijah Yearby: Yearby R. and Mohapatra S. (2021). Systemic Racism, The Government’s Pandemic Response, and Racial Inequities in COVID-19. Emory Law Journal, 70(7), 1418–1473.
Korenman, S., Remler, D. K., & Hyson, R. T. (2019). Medicaid Expansions and Poverty: Comparing Supplemental and Health-Inclusive Poverty Measures. Social Service Review, 93(3), 429–483. https://doi.org/10.1086/705319
Author(s): Sanders Korenman, Dahlia Remler, City University of New York Graduate Center; Rosemary Hyson, City University of New York, Baruch College
Article Type: Peer-reviewed journal
Authors explain how a newly constructed measure of poverty, called the “Health-Inclusive Poverty Measure,” that accounts for both health insurance needs and resources to meet them, builds on the research related to the impact of Medicaid expansion on poverty. The premise for this new measure is that health insurance is a basic necessity and should be incorporated into how poverty is measured. The Census Bureau’s supplemental poverty measure, another common measure of poverty, accounts for indirect effects of health insurance on poverty. Comparatively, the new Health Inclusive Poverty Measure adds insurance needs, does not deduct out-of-pocket spending on premiums, adds health insurance benefits, and caps other deductions, such as deductibles and copays. Using this new measure, the authors explain that Medicaid can move a family out of poverty when their resources are above the measure threshold or keep them from falling into poverty due to out-of-pocket expenses. Authors conduct logistical regressions and show that the poverty rate as defined by the new health-inclusive measure is lower in expansion states than non-expansion states; the deep poverty rate is lower, too, in expansion states versus non-expansion states. Differences were generally smaller and not statistically significant when using the supplemental measure. Thus, the authors conclude that any rollbacks in Medicaid expansion would not only hurt public health, but also increase poverty as well.
Snowden, L., & Graaf, G. (2019). The “Undeserving Poor,” Racial Bias, and Medicaid Coverage of African Americans. Journal of Black Psychology, 45(3), 009579841984412. https://doi.org/10.1177/0095798419844129
Author(s): Lonni Snowden, Health Policy and Management, University of California Berkeley; and Genevieve Graaf, School of Social Work, University of Texas at Arlington
Article Type: Peer-reviewed journal
This article elevates the structural determinants of African American individuals’ physical and psychological well-being, namely stereotypes and biases that deny these individuals much-needed health insurance coverage and treatment. Authors attribute greater African American-White disparity in coverage to African American individuals’ disproportionate residence in states that declined to expand Medicaid. Authors build on earlier research by Colleen Grogan and Sung-geun Ethan Park documenting the association between state’s acceptance of Medicaid expansion and representation of African American people and White peoples’ willingness to accept expansion.* In addition, while stigma associated with Medicaid coverage has lessened for some population groups, it has not for the “non-deserving” poor, i.e., nonelderly, nondisabled adults. In fact, studies suggest that negative attitudes towards Black people explains opposition to welfare spending and public health insurance coverage. Authors call on additional research documenting both the benefits of expansion and how biases act as a barrier. The authors also encourage Medicaid administrators and providers to offer culturally sensitive care.
*Grogan, C. M., & Park, S. (Ethan). (2017). The Racial Divide in State Medicaid Expansions. Journal of Health Politics, Policy and Law, 42(3), 539–572. https://doi.org/10.1215/03616878-3802977
McGregor, B., Li, C., Baltrus, P., Douglas, M., Hopkins, J., Wrenn, G., Holden, K., Respress, E., & Gaglioti, A. (2020). Racial and Ethnic Disparities in Treatment and Treatment Type for Depression in a National Sample of Medicaid Recipients. Psychiatric Services, 71(7), 663–669. https://doi.org/10.1176/appi.ps.201900407
Author(s): Brian McGregor, Glenda Wrenn and Kisha Holden, Department of Psychiatry and Behavioral Sciences & The Satcher Health Leadership Institute, Morehouse School of Medicine, Atlanta, Georgia; Chaohua Li and Peter Baltrus, National Center for Primary Care
Article Type: Peer-reviewed journal
This article explores disparities in uptake and modality of treatment for depression for those who are enrolled in Medicaid and seeking mental health care. Authors analyze data from a nationally representative sample of Medicaid claims (in 28 states and the District of Columbia) from 2008-2009. The study identified that African American Medicaid enrollees diagnosed with depression were about half as likely to have received treatment compared to white Medicaid enrollees diagnosed with depression; Hispanic Medicaid enrollees diagnosed with depression were about three-quarters as likely to have received treatment compared to white Medicaid enrollees diagnosed with depression. Additionally, African Americans who received treatment for their depression were “…less likely to receive medication alone…”, but more likely to only be in therapy (without medication) compared to whites. These findings stood when controlled for medical comorbidities, neighborhood income inequality and poverty, and neighborhood educational context. The authors attribute these disparities partially to cultural differences and stigma of receiving mental health care, as well as provider implicit and explicit bias and structural factors that perpetuate inequities. The authors recommend integrated care models as a way to overcome stigma and improve mental health care access.
Minoff, E. (2020). The Racist Roots of Work Requirements. Center for the Study of Social Policy (pp. 1–33). Center for the Study of Social Policy. https://cssp.org/wp-content/uploads/2020/02/Racist-Roots-of-Work-Requirements-CSSP-1.pdf
Author(s): Elisa Minoff, Senior Policy Analyst at Center for the Study of Social Policy
Article Type: Report
This resource, written by a policy analyst in an advocacy organization, provides a detailed history of work requirements in the U.S. and how these policies are based on a bias that certain people, i.e., Black people, do not want to work. This report also argues that these policies were written to coerce people, primarily Black people, into certain forms of labor thus inflating the standing of White people and putting any assistance available to non-White people at risk. Despite a lack of evidence in favor of these policies for the well-being of all, they continue to be promoted. For example, the Medicaid work requirements under the Trump Administration proved harmful to families; evaluation of the policy in Arkansas’ showed that the Medicaid work requirement led to coverage losses and no employment gains).* The author argues that in order to stop the creation of policies rooted in structural racism, it is important to understand “how we got here.” Beginning with slavery and White enslavers perpetuating racist stereotypes about Black people, the author discusses how this has evolved to public assistance policies requiring primarily Black families to work in low-wage, insecure jobs. “Work requirements not only deny families much-needed assistance, but they also discount much of their labor, ignoring the caregiving work that people provide to their loved ones….” The author advocates for the abolishment of work requirements and the promotion of policies, e.g., higher minimum wage, child care, and paid family leave, that value all work, no matter the setting or wage.
*Sommers, B. D., Goldman, A. L., Blendon, R. J., Orav, E. J., & Epstein, A. M. (2019). Medicaid Work Requirements — Results from the First Year in Arkansas. New England Journal of Medicine, 381(11), 1073–1082. https://doi.org/10.1056/nejmsr1901772
Nolan, L.T., Beckman, A.L., & Sandoe, E. (2020). "How Foundational Moments In Medicaid’s History Reinforced Rather Than Eliminated Racial Health Disparities", Health Affairs Forefront. https://www.healthaffairs.org/content/forefront/foundational-moments-medicaid-s-history-reinforced-rather-than-eliminated-racial-health
Author(s): LaShyra T. Nolen, Founding Executive Director of We Got Us and Current Student Harvard Medical School; Adam L. Beckman, Medical Student at Harvard Medical School and Harvard Business School; Emma Sandoe, Associate Director of Strategy and Planning at North Carolina Medicaid and Adjunct Professor at Duke University
Article Type: Peer-reviewed online brief
The authors examine foundational moments in the history of the Medicaid program—the creation of Medicaid (1965), welfare reform (1996), the ACA Medicaid expansion (2012), and the COVID-19 pandemic (2020)—that led to inequities in access to care as well as the racial disparities and disparate health outcomes that resulted. The authors call for policy changes in Medicaid that focus on: improving access to care for marginalized communities; prioritizing clinical care to address diseases and conditions that have disproportionately affected Black Americans; diversifying the health care and nursing facility workforce; and incentivizing nursing facilities to provide minority patient access to care while also address disparities minority patients often face.
Shafer, P. R., & Ndugga, N. (2020). Fighting the Institutionalization of Racism in Medicaid. American Journal of Public Health, 110(12), 1790–1791. https://doi.org/10.2105/AJPH.2020.305946
Author(s): Paul R. Schafer, Professor at Boston University School of Public Health; Nambi Ndugga, Policy Analyst at the Kaiser Family Foundation’s Racial Equity and Health Policy Program
Article Type: Peer-reviewed journal perspective
This American Journal of Public Health Perspective written at the height of the COVID-19 pandemic by scholars at Boston University raises concerns about some states using flexibilities offered in the Medicaid program to exacerbate inequities. The authors cite the Trump Administration initiatives restricting benefits and spending (such as converting Medicaid to a block grant, work requirements, and restrictions on retroactive eligibility) as having a disproportionate negative effect on Black Americans and people of color. The authors move on to caution decision makers against promoting rather than reversing institutional racism in initiatives like these. These initiatives, regardless of if they were established with racist intent or not, demonstrate that inequities are still built into Medicaid’s policies and practices today – and that we need to replace them with equitable policies that benefit those most in need.
Jaramillo, E. T., & Willging, C. E. (2021). Producing insecurity: Healthcare access, health insurance, and wellbeing among American Indian elders. Social Science & Medicine, 268. https://doi.org/10.1016/j.socscimed.2020.113384
Author(s): Elise Trott Jaramillo, Associate Research Scientist at the Pacific Institute for Research and Evaluation (PIRE-Southwest); Cathleen Willging, Center Director and Senior Research Scientist II at the Pacific Institute for Research and Evaluation (PIRE-Southwest)
Article Type: Peer-reviewed journal
This peer-reviewed article provides a qualitative perspective on the experiences of Native American elders in the health care system across the United States. Native American people have experienced significantly higher rates of mortality from heart disease, higher rates of diabetes and mental health concerns, and have the lowest life expectancy of any aggregated race in the country. This is attributed to the lack of sufficient funding for the Indian Health Service, a separate health system that is meant to serve enrolled members of federally recognized tribes. While the expansion of Medicaid and other provisions under the Affordable Care Act (ACA) improved access to health insurance coverage for American Indian people, concerns of inadequate services sparked this research study, which consisted of semi-structured interviews with 95 elders between June 2016 and March 2017. The study found the elders lacked confidence in three main aspects of the health care system: interactions with providers (e.g., lack of trust, accessible communication, and/or coordination); identification of health insurance coverage and health care costs (e.g., confusion); and federal policy for American Indians. The authors conclude with a call to action to address health care hesitancy in a way that does not increase the complexity that Native people already face in navigating the health care system, but instead focuses resources on systemic and provider-centric changes that can build confidence for American Indian people seeking care.
Alio, A. P., Wharton, M. J., & Fiscella, K. (2022). Structural Racism and Inequities in Access to Medicaid-Funded Quality Cancer Care in the United States. JAMA Network Open, 5(7). https://doi.org/10.1001/jamanetworkopen.2022.22220
Author(s): Paula Amina Alio, Professor in the Department of Public Health Sciences at the University of Rochester; Mitchell J. Wharton, Associate Professor of Clinical Nursing and Associate Dean for Equity and Inclusion at the University of Rochester; Kevin Fiscella, Professor in the Departments of Family Medicine and Public Health Sciences at the University of Rochester
Article Type: Commentary
Authors in this commentary share their perspectives on findings from a secret shopper study building off of the established association between having Medicaid coverage and a lower likelihood of scheduling specialty care appointments compared to those with private insurance coverage. In that secret shopper study from Marks et al*, researchers found that only two thirds of facilities accepted new patient appointments for cancer treatment for patients covered by Medicaid. Authors of this commentary suggest that downstream solutions, including improved reimbursement and adoption of new payment models, are not enough to help resolve these issues of access to care. They aim to raise awareness of structural racism in health care and promote equity-centered health care policies over those that only advantage white populations. Examples of the authors’ suggested solutions include Centers for Medicaid Services (CMS) requiring facilities to make their Medicaid policies public as well as incorporating ‘access to Medicaid’ in managed care and accreditation organizations requirements and standards. Improving data collection, gathering patient experience exit surveys, and establishing patient grievance processes were also proposed as possible solutions.
*Marks, V., Hsiang, W., Nie, J., Demkowicz, P., Umer, W., Haleem, A., Galal, B., Pak, I., Kim, D., Salazar, M. C., Berger, E. R., & Leapman, M. (2022). Acceptance of Simulated Adult Patients With Medicaid Insurance Seeking Care in a Cancer Hospital for a New Cancer Diagnosis. JAMA Network Open, 5(7), e2222214–e2222214. https://doi.org/10.1001/jamanetworkopen.2022.22214
Somers, S., & Perkins, J. (2022). The Ongoing Racial Paradox of the Medicaid Program. Journal of Health and Life Science (pp. 96–112). American Health Law Association. https://healthlaw.org/wp-content/uploads/2022/05/The-Ongoing-Racial-Paradox-of-the-Medicaid-Program.pdf
Author(s): Sarah Somers, Managing Attorney of the National Health Law Program’s (NHeLP) Chapel Hill, North Carolina Office; Jane Perkins, Legal Director of the National Health Law
Program (NHeLP)
Article Type: Peer-reviewed journal
This resource discusses the history of Medicaid and makes key observations about the paradox of the Medicaid program – that while Medicaid has decreased disparities in health insurance coverage and access among the poor and people of color, the program was also founded on inherently racist premises. The authors point to three distinct Medicaid policies that shaped its weaknesses. First, the program’s beginnings were not federal; it was an optional state-level program. This resulted in disparities between states, as the authors say, “States in the South lagged. Thirty-two states had adopted Medicaid before even the first former Confederate state had adopted it.” The second major issue with Medicaid’s foundations that authors call out was its roots in the voluntary health coverage program under the Kerr-Mills Act of 1960, which had the stigma of a welfare program. The authors point out that in order, “to qualify, a person had to be poor and fit with a population group deemed worthy of coverage.” The third major concern with Medicaid’s history according to these authors is its fundamental coverage, delegation of decision making, and enforcement of covered services to states. Despite protections afforded under Title VI of the Civil Rights Act, extremely segregated facilities and disparities in both services and outcomes exist to this day. Authors discuss ways Medicaid can address systemic racism, including encouraging the expansion of Medicaid in states that have not yet made that decision, the addition of requirements to improve health equity in state contracts with Medicaid managed care plans, and the improvement of collection and reporting of disaggregated data.
Wallace, J., Lollo, A., Duchowny, K. A., Lavallee, M., & Ndumele, C. D. (2022). Disparities in Health Care Spending and Utilization Among Black and White Medicaid Enrollees. JAMA Health Forum, 3(6), e221398. https://doi.org/10.1001/jamahealthforum.2022.1398
Author(s): Jacob Wallace, Professor at Yale School of Public Health, Anthony Lollo, Professor at Yale School of Public Health, Kate Duchowny, University of California – San Francisco, Chima Ndumele, Professor at Yale School of Public Health, Matthew Lavallee, Yale University.
Article Type: Peer-reviewed journal
This article utilizes 2016 administrative records from three Southern and Midwest state Medicaid programs to compare whether there were differences in health care spending and utilization between nearly two million black and white Medicaid enrollees. Results indicated that spending on adult Black enrollees was less than adult white enrollees after adjusting for demographic characteristics and health status. Additionally, Black Medicaid adults and children utilized health care less, including primary care, but visited the emergency department more than white Medicaid populations. Regarding preventive care, Black enrollees had higher rates of measures of some screenings, e.g., breast cancer, cervical cancer, chlamydia, than white enrollees. However, Black enrollees with asthma, diabetes, and cardiovascular conditions filled fewer pharmaceutical prescriptions than white enrollees. The authors attributed these differences in part to the structural and interpersonal racism that racial and ethnic minority groups face when navigating the health care system, as well as reduced access to care despite coverage increases for racial minorities overall. The authors recommend improvements to Medicaid managed care risk adjustment practices as Black enrollees are currently undercompensated in coverage due to unmet need. In addition, authors suggest a need to align plan and provider incentives to address health equity in the Medicaid program.
Goran, A., Tatum, L., Brumfield, C., & Carr, A. (2023). Re-Envisioning Medicaid & CHIP as Anti-Racist Programs. Georgetown Center of Poverty and Law. https://www.georgetownpoverty.org/wp-content/uploads/2023/06/Re-envisioning-Medicaid-CHIP-June2023.pdf
Author(s): Ayan Goran, Policy Analyst at the Georgetown Center on Poverty and Inequality (GCPI); Laura Tatum, Managing Director of Policy & Research at GCPI; Cara Brumfield, Director of Income and Work Supports at the Center for Law and Social Policy (CLASP); Aileen Carr, Interim Executive Director of GCPI
Article Type: Report
This report discusses how many aspects of the Medicaid and Children’s Health Insurance Program (CHIP) programs contribute to health inequities among enrolled people of color. The report covers key historical factors, such as the low reimbursement rates to hospitals and clinics for services, continued racial segregation in nursing facilities, and limited coverage for birthing people and their newborns. The latter likely contributes to the United States’ maternal mortality rate ranking highest among developed countries. The authors also specifically emphasize systemic and administrative barriers in the enrollment process, highlighting political and media narratives that have resulted in exclusionary policies directed toward single mothers of color, particularly black women, as well as immigrants. Work requirements were another key exclusionary factor, as well as a quick turnaround on verification processes that relied on paper mail to arrive at the correct address in a timely manner among other administrative burdens. This report provides multiple recommendations on how to address these issues within both Medicaid and CHIP, including taking action at the federal level to close the coverage gap both in states that have not expanded Medicaid and for certain populations, making CHIP funding permanent, increasing Medicaid reimbursement rates, and alleviating administrative burdens. Additionally, authors point to centering community voices and empowering program participants through partnerships with community advocacy organizations and community health workers, compensating these organizations and/or individuals for their time.
Haeder, S. F., & Moynihan, D. P. (2023). Race and Racial Perceptions Shape Burden Tolerance for Medicaid and the Supplemental Nutrition Assistance Program. Health Affairs, 42(10), 1334–1343. https://doi.org/10.1377/hlthaff.2023.00472
Author(s): Simon Haeder, Department of Health Policy & Management, Texas A & M University; Donald Moynihan, School of Public Policy, Georgetown University
Article Type: Peer-reviewed journal
This piece uses survey data to explore the relationship between racial resentment and public attitudes towards administrative policies in public programs such as Medicaid and the Supplemental Nutrition Assistance Program (SNAP). A random sample of adults with either Medicaid or SNAP were surveyed about the effects of administrative burdens (i.e., requiring in person interviews, lack of presumptive eligibility, lack of express lane eligibility, more frequent renewals, work requirements, and lack of continuous coverage) on program enrollment; a treatment group received additional information on how administrative burdens affect certain populations or exacerbate racial inequities in the survey introduction, while a control group did not receive this additional information. Authors found no relationship between exposure to this information and support for state actions associated with each of the six types of administrative burden. However, authors did find a relationship between support for administratively burdensome policies and racial resentment. Based on an analysis of non-Hispanic white respondents who were asked about racial resentment toward Black people, those with higher levels of racial resentment were more supportive of Medicaid-specific policies that would create burden. Implications for policy makers, according to the authors, include that the general public’s views on how state actions affect different socioeconomic groups are very important to the legislative process, and these views have an impact on support for new or proposed policies. However, it is also important to note that the finding that the public is hesitant to reduce initial enrollment burdens (such as work requirements) may be due to concerns of program integrity and combating fraud in addition to racial resentment. Overall, the public is more supportive of policies that reduce burden after enrollment, such as less frequent renewals and elimination of in-person interview requirements.
Ku, L. (2023). Medicaid And SNAP Advance Equity But Sometimes Have Hidden Racial And Ethnic Barriers. Health Affairs, 42(10), 1347–1350. https://doi.org/10.1377/hlthaff.2023.00994
Author(s): Leighton Ku, Professor and Director of the Center for Health Policy Research at the Milken Institute School of Public Health, George Washington University
Article Type: Perspective in peer-reviewed journal
The author provides the historical context for programs like Medicaid and SNAP, explaining how they fill a gap in services for individuals and households living in poverty and addressing disparities in access to health care and food. While progress has been made, these programs are currently operating in an environment that runs counter to their original goals. While not explicitly racist, certain administrative policies (such as work requirements and immigration status restrictions), can be implicitly so, as they often have a disproportionately negative effect on specific populations of color. The author recommends that agencies administering these programs should reconsider policies that hinder enrollment and benefits.
Michener, J., & Ford, T. N. (2023). Racism and Health: Three Core Principles. Milbank Quarterly, 101(S1), 333–355. https://doi.org/10.1111/1468-0009.12633
Author(s): Jamila Michener, Professor of Government and Public Policy, Co-Director of the Center of Health Equity at Cornell University*; Tiffany N. Ford, Brookings Institution at University of Illinois at Chicago
Article Type: Peer-reviewed journal
This article discusses the important context of racism and three core principles that the authors see as key to understanding and implementing policy changes related to health and racial equity. Those three core principles are described as: “interlocking systems of oppression”, “cumulative disadvantage”, and “power”. Racism operates both alongside and interlocked with other systems of oppression, such as patriarchy, structural sexism, ageism, sizeism, ableism, homophobia, and others, which have impacted society both historically and in the present day by shaping the ways in which people live. Racist and oppressive policies can have a cumulative negative effect (“cumulative disadvantage”) across systems (examples of such systems include “child welfare, public assistance, banking, incarceration, employment, housing”), and generally throughout one’s life course. The authors state that studying and addressing policies in these areas in isolation is not productive – “people and communities experience these policy arenas as overlapping aspects of daily life” just as they experience many “interlocking systems of oppression” at once. The authors also discuss the complex relationship between the concepts of power and race, arguing that power fuels racism. Race, the authors say, is not a biological fact, but rather a social construct based on appearances. And power, according to the authors, is based on where a group falls on a socially constructed racial hierarchy. Thus, power fuels racism, as groups in power will act to both construct and maintain systems that perpetuate inequities and keep themselves at the top of the hierarchy. The Medicaid program is discussed by the authors as having many policies that perpetuate these differences between races and create both cumulative disadvantage and power imbalances, with work requirements used as a prime example. The authors suggest that progress towards a more equitable future for everyone requires program design, policymaking, data collection, and research that both collaborates with and centers communities experiencing inequities. The authors also propose engaging professionals in various disciplines, such as public health, public policy, and urban planning, as well as different sectors of organizations such as academia, government, and non-profits, in the creation and revision of equitable policies and programs.
*Other resources from Jamila Michener include her book, Fragmented Democracy: Medicaid, Federalism, and Unequal Politics, as well as this Vox article on the politics and policy of racism in American health care.
[1] State Health & Value Strategies (SHVS). (2021). Talking about anti-racism and health equity: Discussing racism. https://www.shvs.org/wp-content/uploads/2021/08/Talking-About-Anti-Racism-Health-Equity-1-of-3.pdf