 VISIT STATE HEALTH COMPARE
VISIT STATE HEALTH COMPARE
Blog & News
Au-Yeung, Caroline
Worrall, Christina




SHADAC Brief Examines Minnesota's Accountable Communities for Health
October 15, 2019:SHADAC researchers released a new brief that provides the context surrounding the development and implementation of Minnesota’s Accountable Communities for Health, or ACHs, and describes key components of ACH models implemented across the state. The following are highlights from the brief.
ACHs: Defined
Minnesota's ACHs are community-led models of delivering medical and non-medical care and services to improve the health of a target population with substantial health and social needs. ACHs bring together diverse community partners, driven by the specific needs of the target population and the prevailing health and social conditions in the community. [1] The state awarded grants to fund the creation of 15 ACHs under the federal State Innovation Model (SIM) Initiative.
ACH Requirements
Core requirements for ACHs were to (1) establish a collaborative leadership structure that involved community partners; (2) develop and implement a community-based care coordination system or team; and (3) implement a population-based health prevention plan. Other key elements of Minnesota’s ACH model include a sustainability plan, a measurement plan, and participation in Learning Collaborative and evaluation activities.
ACH Characteristics
-
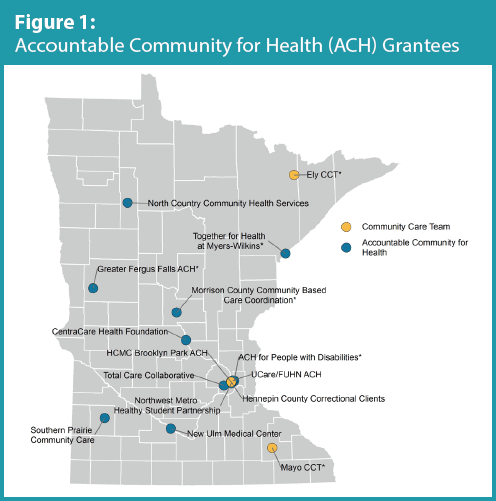
In all, eight ACHs were anchored in urban areas, six were located in rural areas, and one had both an urban and rural presence (Figure 1).
-
Three of the ACHs were outgrowths of an earlier Minnesota grant program, called the Community Care Team (CCT) pilot, which was administered from 2012 to 2013 by the Minnesota Department of Health’s patient-centered medical home initiative and was meant to expand beyond the medical focus of health care homes.
-
Eight ACHs established care coordination models that focused broadly on the medical and social needs of their target populations without regard to a specific category of health condition; four were focused on mental and behavioral health (e.g., depression, substance abuse, serious and persistent mental illness, etc.) within their target populations; and three focused on specific or comorbid chronic medical conditions within their target populations.
ACH Leadership and Partners
-
In all, ACHs identified 279 organizational partners, including partners who held both leadership and operational roles. The number of partners involved in any individual ACH ranged from six to 34.
-
In nearly all (14) ACHs, an Accountable Care Organization (ACO) representative or provider participant served on the ACH Leadership team. When the ACH target population overlapped, select ACO partners provided data, data analytics, and connections with providers and have been a source of patients/referrals for the ACHs.
-
Two-thirds (10) of ACHs involved a local public health partner in their work. ACHs with a public health partner reported that public health organizations brought a health promotion focus, hired key coordination staff, conducted population health activities, contributed data and evaluation expertise, and supported community engagement and relationship building.
-
Nine ACHs included at least one community or target population member on their leadership teams.
ACH Community-Based Care Coordination Systems or Teams
-
Because of the flexibility of the ACH program, as a result of which the ACHs were working with a broad range of target populations across a variety of settings, no single care coordination model accurately captures the various ACH care coordination approaches. Instead, ACH care coordination models can best be conceptualized by looking at the locus/anchor of care coordination and the intensity of care coordination services provided.
-
Nine ACHs conducted care coordination from the starting point of a medical facility or organization (clinic, hospital, health plan); four initiated care coordination within a community organization (social service agency, school, group living community); and two used a combination of medical and community-based starting points.
-
The care coordination efforts of about half of the ACHs fall at multiple points along a continuum of intensity that increases in tandem with patient needs. In these cases, services ranged from the provision of information and resources to a referral and/or handoff to an extensive wraparound. Other ACHs tended to concentrate their work at certain points along the continuum, depending largely on the needs of their target populations. Four ACHs, for example, targeted particularly high-need individuals such as those with developmental disabilities and mental illness, and therefore focused on high-intensity coordination work.
-
ACHs varied in terms of care coordination reach, with the average number of individuals reached per quarter by a given ACH ranging from fewer than 100 to more than 300 in 2016.
ACH Population-Health Based Prevention Plans
-
In developing their population-based prevention plans, ACHs frequently built upon prevention work intiatied or underway through other community efforts. For example, six ACHs leveraged the Statewide Health Improvement Program, three leveraged Community Transformation Grants, and nine leveraged other local public health initiatives.
-
All ACHs focused in whole or in part on the same populations for both their care coordination and population health components, with frequent overlap between care coordination and population health activities.
-
Where data was provided/available, ACHs reported reaching anywhere from 201 to 3,000 individuals each through population health programming and activities.
Funding: The Federal SIM Initiative
ACHs in Minnesota were funded through a $45 million state’s State Innovations Model (SIM) cooperative agreement, awarded to the Minnesota Department of Human Services in 2013 by the Center for Medicare and Medicaid Innovation (The CMS Innovation Center). Administered by the Minnesota Departments of Health and Human Services, the funding was used to implement the Minnesota Accountable Health Model Framework, for which SHADAC was the state evaluator.
State-Led Evaluation: SHADAC
The Innovation Center required a federal multistate evaluation of the SIM initiative as well as individual state evaluations. The Minnesota Department of Human Services contracted with SHADAC to design and conduct the state evaluation of Minnesota’s SIM initiative. The evaluation was conducted between 2015 and 2017. The results of this evaluation are not endorsed by the federal government. These findings do not reflect the views of and may differ from the federal government’s evaluation.
[1] Awsumb, B., Dobbe, C., Ly-Xiong, S., Rodriguez-Hager, R., Rydrych, D., & Terrill, W. (October 2016). "Accountable Communities for Health: Perspectives on Grant Projects and Future Considerations." Retrieved from http://www.dhs.state.mn.us/main/groups/sim/documents/pub/dhs-290682.pdf

